- Visibility 76 Views
- Downloads 17 Downloads
- DOI 10.18231/j.jco.2023.031
-
CrossMark

Accuracy of lab scanners in establishing dental measurements: In-vitro study
- Author Details:
-
 Prairna Zaroo Kalia *
Prairna Zaroo Kalia *
-
Sonal Attri
-
Vaibhav Misra
-
Divya Joshi
-
Ashish Yadav
-
Sumit Kalia
Introduction
The use of study models in orthodontics has been acknowledged as an essential and important component of the specialty. Traditionally, plaster orthodontic models, direct measurements, 2D images, and radiographs [1] have been employed for obtaining information.
Digital images and 3D models are increasingly used as orthodontic record in numerous practices throughout the world in order to enhance the efficacy and accuracy of the record- taking. The orthodontist can do standard measurements and acquire various analyses from the digitalized models.[2]
The published material contains inconsistent information about the precision of dental dimensions obtained from digital models generated via scanning plaster models and provides scant information about digital models created by scanning impressions. Additionally, there are no studies that evaluate the dependability and correctness of model analysis performed on 3D models created from dental impressions made using rubber base impression material.
Determining the accuracy of the measurements taken by the lab scanner on rubber-based impressions, the scanned stone cast, and the traditional stone cast by digital vernier calliper was the intent of this study.
The goals of this research were to compare accuracy between measurements made
On a stone cast manually by a digital vernier calliper.
On the same stone cast by a lab scanner.
On the impression by a lab scanner.
Materials and Methods
Source of Data: This study was carried out on patients in the Department of Orthodontics and Dentofacial Orthopaedics at Divya Jyoti (D.J) College of Dental Science and Research, Modinagar. U.P.
Sample design: In-vitro study
Study period: 1 year
Sample size: 20
Inclusion criteria
No prior orthodontic treatment history.
No missing tooth anterior to first molars.
Absence of supernumerary tooth.
Patients with all permanent teeth.
Exclusion criteria
Congenital anomalies
Grossly decayed teeth
Congenitally missing teeth
Fractured teeth
Caries involving proximal surfaces
Presence of retained deciduous teeth
Materials and Methods
Maxillary perforated impression trays ([Figure 1])
Rubber base impression material (Condensation C silicone elastomeric impression material ([Figure 2])
Type III Dental stone ([Figure 3])
Digital calliper (DIGE 150-3V Battery ([Figure 4])
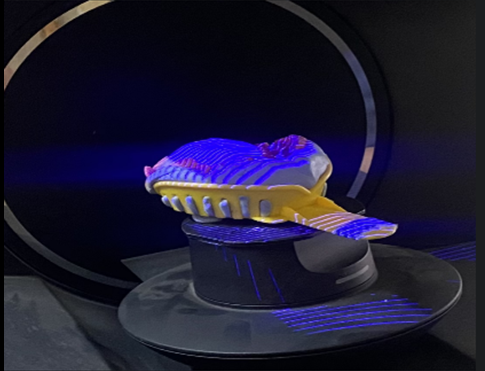
Lab scanner (3 shapes series E3 1tb1920033b ([Figure 5])
Software for 3 D Analysis (3 Shapes Ortho analyzer software version 2019)
Methodology
Two sets of maxillary rubber base impressions were taken from 20 random patients in our department. Impressions were disinfected by immersion in diluted hypochlorite solution followed by rinsing the impression adequately.
Following that, the samples were split into three groups:
Group A: Manual measurement of the stone cast The stone cast poured from the first rubber base impression, was measured manually employing a digital vernier a calliper with a 0.01 mm accurateness ([Figure 6]).
Group B: Direct scan of the impressionThe second rubber base impression was measured by the lab scanner ([Figure 7]).
Group C: Scanned stone castThe lab scanner was used to scan and measure the stone casts utilized in group A ([Figure 8]).
In the present study, the following metrics have been utilized:
Mesio-distal width, Intercanine Distance, Inter first premolar width, Inter second premolar width, Intermolar width, Arch Perimeter, Arch length, Buccolingual width and Clinical crown height.
Statistical Tests
Each parameter was measured in 3 Shapes ortho analyzer software version 2019.




A power analysis was performed; For an 80% likelihood, 20 models per category were needed, with a standard deviation of 0.2 mm and a variance of 0.18 predicted. The IBM Statistical Package for Social Services (SPSS) version 21 program was used to modify the measurements once they had been gathered, saved, and stored in Excel. Descriptive statistics were generated. The one-way ANOVA technique (Analysis of Variance) was used for the statistical analysis of all measurements. The significance level was 5%.
Results
Descriptive statistics
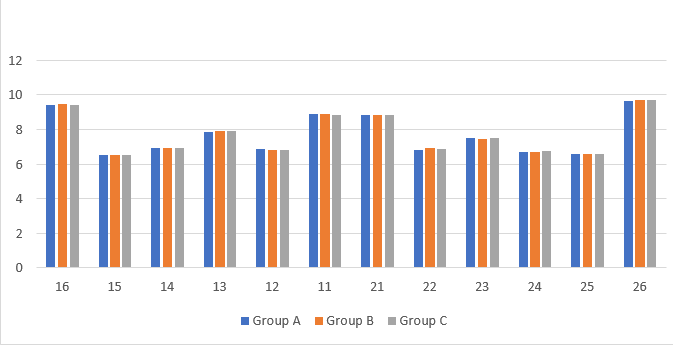
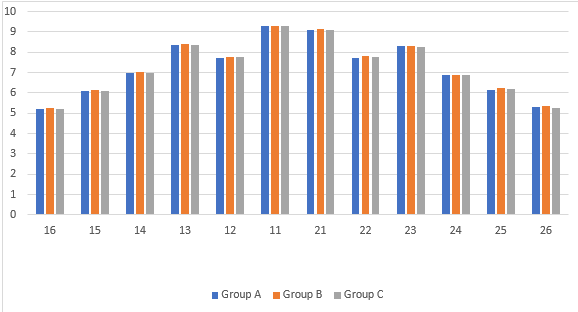
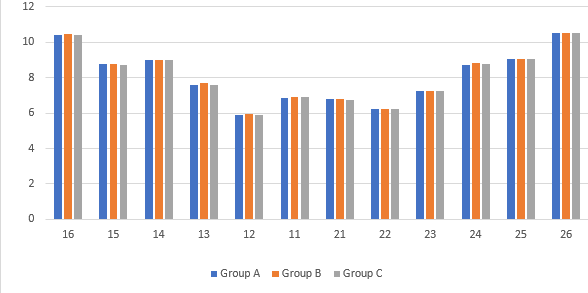
Descriptive statistics depicts that there was no statistically significant difference between the mean mesiodistal width, mean clinical crown height, mean buccolingual width, the mean of inter canine, inter first premolar, inter second premolar, inter molar distance, arch perimeter & arch length of all the three groups. Graph 1, Graph 2, Graph 3 depict the mean mesiodistal width, mean clinical crown height and mean buccolingual width of group A, Group B and Group C.
Inferential statistics
Inferential statistics show that the One-way ANOVA test for mesio-distal width, clinical crown height, buccolingual width inter canine, first premolar, second premolar, molar distance, arch perimeter & arch length between Group A, Group B and Group C showed no statistically significant difference.
|
Between Group A, Group B and Group C |
||||||
|
|
Sum of Squares |
Degrees of Freedom |
Mean Square |
F Value |
P Value |
|
|
ICD |
Between Groups |
0.129 |
3 |
.504 |
0.996 |
.40 |
|
Within Groups |
8.050 |
57 |
.141 |
|
|
|
|
Total |
9.179 |
59 |
|
|
|
|
|
IFPM |
Between Groups |
.113 |
2 |
.057 |
1.829 |
.170 |
|
Within Groups |
1.768 |
57 |
.031 |
|
|
|
|
Total |
1.881 |
59 |
|
|
|
|
|
ISPM |
Between Groups |
.014 |
2 |
.007 |
.014 |
.986 |
|
Within Groups |
29.232 |
57 |
.513 |
|
|
|
|
Total |
29.246 |
59 |
|
|
|
|
|
IMD |
Between Groups |
.431 |
2 |
.215 |
.062 |
.940 |
|
Within Groups |
196.818 |
57 |
3.453 |
|
|
|
|
Total |
197.249 |
59 |
|
|
|
|
|
AP |
Between Groups |
.005 |
2 |
.003 |
.000 |
1.000 |
|
Within Groups |
2449.115 |
57 |
42.967 |
|
|
|
|
Total |
2449.120 |
59 |
|
|
|
|
|
AL |
Between Groups |
.004 |
2 |
.002 |
.000 |
1.000 |
|
Within Groups |
445.111 |
57 |
7.809 |
|
|
|
|
Total |
445.114 |
59 |
|
|
|
Discussion
Because of the drawbacks of plaster models, which until recently were rated as the gold standard in treatment planning, digital models have been acknowledged as a replacement.[3]
Studies by Stevans DR et al. (2006)[4] and Zilberman O et al. (2003)[5] indicated that measurements taken from digital models had a high degree of reproducibility, reliability, and validity. Only a few investigations on the accuracy of linear measurements done on digital models and gold standard plaster models were accessible, including those by Camardella LT et al (2020), [6] Keating AP et al (2008), [7] Kiviahde H et al (2017), [8] Bell A et al (2003),[9] Sakar T et al (2017), [10] and Kim J et al (2014).[11] Therefore, we did this study to compare the accuracy of measurements made on conventional stone casts by digital vernier calliper to measurements made on digital models created by lab scanning of rubber-based impressions and stone casts.
The study's sample size was established at 20, which seemed sufficient because it was significantly larger than the estimated minimum and was comparable to earlier research by Zilberman O et al (2003)[5] and Santoro M et al (2003).[12] The study's inclusion criteria were in line with earlier research by El-Zanty HM et al (2010). [13] According to Sousa MVS et al (2012), [14] tooth crowding has been observed to make it difficult to perform linear measurements on dental casts, which has led to its exclusion in certain prior studies as the ones by Wiranto MG et al (2013), [15] Yoon JH et al (2018), [16] and Hassan WNW (2016). [17] We chose to include crowding in our study because it is a type of malocclusion that orthodontists regularly deal with.
Our study's conclusions revealed that there was great agreement in linear dental measurements between stone casts and digital models. No statistically significant changes were discovered when the measurements between the manual and digital models were evaluated using the descriptive statistics. The results of the one-way Anova test likewise demonstrated that there was no statistically significant difference between the three groups. The result of our study was consistent with the studies done by Kim J et al (2016), [11] Kiviahde H et al (2017), [8] Labib MA et al (2020) [3] and Camardella LT et al (2020).[6]
In the earlier research undertaken by Verma et al (2019), [18] Santoro M et al (2003) [12] and Gayasso SIJ et al (2018) [19] the comparisons between digital and plaster models resulted in significant differences in some parameters. Contrarily, Abizadeh N et al (2012)[20] discovered parameters with good repeatability and reproducibility when taking into account both digital and manual procedures, which is consistent with the current investigation. These parameters included inter-canine and inter-molar widths, where it was simpler to locate landmarks.
In the work of Verma et al (2019), [18] the maxillary canines' mesiodistal values on digital models typically revealed highest variance and should be taken into account with caution during measurement. The dimensions may not be accurate because of the canine region's curved arch. Considering the excellent surface detail reproduction on the models created by pouring a more dimensionally stable and accurate rubber base impression material in comparison to the alginate used by Verma et al. (2019), our study did not find any statistically significant differences in the mesiodistal measurement of canines.
Also, measurement errors which could have been there were taken care by clearly stating that landmarks and their extensions.
In a prior study, Santoro M. et al. (2003)[12] came to a finding that the estimations of tooth width for each of the measured teeth varied between the plaster and digital model groups. The digital measures were smaller than their counterpart. They suggested that the shrinking of the alginate during shipping and the various pouring times could be responsible for this result. Due to the inclusion of a dimensionally more stable rubber base imprint material, our study could readily avoid these mistakes.
Additionally, in our study, many scans of the same model were taken from various angles in order to achieve more accurate scans. The data from each of these scans was then combined using specialized software (3shape ortho analyser) to a model.
Scanned digital models still have some practical limits when used in orthodontic settings. It can be time-consuming and laborious to scan existing models, which big clinics and institutes might have in plenty. The software's steep learning curve and myriad visualization tools could result in measurement errors. The protection of electronic file data is a different issue. Access to digital study models should be password-protected, as with all other patient records, and for further protection, scanned models should only be transferred with a numbered reference so that the model remains anonymous.[20]
Insolvency of the maker, failure of the computer or software, or other dangers linked with digitalization could render the models permanently or for an extended period of time inaccessible. The biggest financial drawback of digital models is their expensive price.
Our study does have some limitations. Accurate point placement proved challenging despite the software's rotation and magnification features. Because we restricted our investigation to maxillary models, we were unable to assess interarch metrics like overbite and overjet.
The clinical accuracy and dependability of recently launched scanning hardware and software should be evaluated in the future. Along with this, the factors that haven't been fully taken into account in the literature thus far include related expenditures, the amount of time needed, and the preferences of the patient. We must recognize that human error can undermine the accuracy of many measures. We need multiple innovations across a wide range of sectors to overcome this significant issue.
Conclusion
It is safe to claim that digital models can be extremely accurate and valuable in the clinical setting when utilized in conjunction with clinical data and other diagnostic tools.
Source of Funding
None.
Conflict of Interest
None.
References
- DD Moreira, BF Gribel, GDR Torres, KDF Vasconcelos, DQD Freitas, GMB Ambrosano. Reliability of measurements on virtual models obtained from scanning of impressions and conventional plaster models. Braz J Oral Sci 2014. [Google Scholar]
- N Brusco, M Andreetto, L Lucchese, S Carmignato, GM Cortelazzo. Metrological validation for 3D modeling of dental plaster casts. Med Eng Phys 2007. [Google Scholar]
- MA Labib, AR El-Beialy, KH Attia. Evaluation of the accuracy of digital models obtained using intraoral and extraoral scanners versus gold standard plaster model (diagnostic accuracy study). Open Med Imaging J 2020. [Google Scholar]
- DR Stevens, C Flores-Mir, B Nebbe, DW Raboud, G Heo, PW Major. Validity, reliability, and reproducibility of plaster vs digital study models: comparison of peer assessment rating and Bolton analysis and their constituent measurements. Am J Orthod Dentofac Orthop 2006. [Google Scholar]
- O Zilberman, J Huggare, KA Parikakis. Evaluation of the validity of tooth size and arch width measurements using conventional and three-dimensional virtual orthodontic models. Angle Orthod 2003. [Google Scholar]
- LT Camardella, EM Ongkosuwito, EW Penning, AM Kuijpers-Jagtman, OV Vilella, KH Breuning. Accuracy and reliability of measurements performed using two different software programs on digital models generated using laser and computed tomography plaster model scanners. Korean J Orthod 2020. [Google Scholar]
- AP Keating, J Knox, R Bibb, AI Zhurov. A comparison of plaster, digital and reconstructed study model accuracy. J Orthod 2008. [Google Scholar]
- H Kiviahde. Inter-arch digital model vs. manual cast measurements: Accuracy and reliability. Cranio 2017. [Google Scholar]
- A Bell, AF Ayoub, P Siebert. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J Orthod 2003. [Google Scholar]
- T Sakar, K Orhan, A Sinanoglu, O Tosun, U Oz. Assessment of the Accuracy of Orthodontic Digital Models in Dental Education. Eurasia J Math Sci Technol Educ 2017. [Google Scholar]
- J Kim, MO Lagravere. Accuracy of Bolton analysis measured in laser scanned digital models compared with plaster models (gold standard) and cone-beam computer tomography images. Korean J Orthod 2016. [Google Scholar]
- M Santoro, S Galkin, M Teredesai, OF Nicolay, TJ Cangialosi. Comparison of measurements made on digital and plaster models. Am J Orthod Dentofac Orthop 2003. [Google Scholar]
- HM El-Zanaty, AR El-Beialy, A El-Ezz, AM Attia, KH El-Bialy, AR Mostafa. Assessment of the accuracy of a three-dimensional imaging system for archiving dental study models. J Orthod 2003. [Google Scholar]
- MV Sousa, EC Vasconcelos, G Janson, D Garib, A Pinzan. Accuracy and reproducibility of 3-dimensional digital model measurements. Am J Orthod Dentofac Orthop 2012. [Google Scholar]
- MG Wiranto, WP Engelbrecht, HE Nolthenius, WJ Van Der Meer, Y Ren. Validity, reliability, and reproducibility of linear measurements on digital models obtained from intraoral and cone-beam computed tomography scans of alginate impressions. Am J Orthod Dentofac Orthop 2013. [Google Scholar]
- JH Yoon, HS Yu, Y Choi, TH Choi, SH Choi, JY Cha. Model analysis of digital models in moderate to severe crowding: in vivo validation and clinical application. Bio Med Res Int 2018. [Google Scholar] [Crossref]
- W Hassan, SA Othman, CS Chan, R Ahmad, SN Ali. Abd Rohim A. Assessing agreement in measurements of orthodontic study models: Digital caliper on plaster models vs 3-dimensional software on models scanned by structured-light scanner. Am J Orthod Dentofac Orthop 2016. [Google Scholar]
- RK Verma, SP Singh, S Verma, V Kumar, NR Bhupali, S Arora. Comparison of reliability, validity, and accuracy of linear measurements made on pre- and posttreatment digital study models with conventional plaster study models. J Orthod Sci 2019. [Google Scholar]
- S Gayosso. Difference between manual and digital measurements of dental arches of orthodontic patients. Medicine 2018. [Google Scholar]
- N Abizadeh, DR Moles, O Neill, J Noar. Digital versus plaster study models: how accurate and reproducible are they?. J Orthod 2012. [Google Scholar]