Introduction
Soft tissue, skeletal relationship and dental relationship after tracing the cephalogram have been used and considered as an essential tool for diagnosis during case discussion and for evaluation of a proper treatment plan for orthodontic treatment. It is very crucial to understand that soft tissue drape may be misleading in diagnosis and treatment plan of malocclusion. Also Angle’s classification masks the underlying skeletal maIocclusion.1, 2, 3, 4 So it is very important to analyse these two aspects of treatment planning that is Soft Tissue analysis especially LIP THICKNES and to diagnose the underlying Skeletal Malocclusion present in Angle’s class I malocclusion .So the most important parameter would be correlating the lip thickness with Angle’s class I malocclusion and its underlying skeletal malocclusion. Many studies have investigated the effect of orthodontic treatment on the facial profile have focused on predicting lip response relative to incisor movement. For the diagnosis and treatment planning of malocclusions, the skeletal malocclusion is evaluated by the antero - posterior (AP) jaw relationship which is an important step, and this relationship is generally determined by cephalometric analysis. The 'Wits' analysis, was first described by Jacobson (1975, 1976) at the University of the Witwatersrand, South Africa, hence the name 'WITS’.5 But still sagittal jaw relationships are difficult to evaluate because of rotations of the jaws during growth, vertical relationships between the jaws and the reference planes, and a lack of validity of the various methods proposed for their evaluation (Jacobson, 1975 ; Moyers et al. , 1979 ; Baik and Ververidou, 2004 ; Nanda, 2005 ). Wits appraisal was used to overcome the existing limitations of angle ANB (Jacobson, 1975). In Wits appraisal we don’t use nasion so it reduces the rotational effects of jaw growth, but it uses the occlusal plane, which is a dental parameter, to describe the skeletal discrepancies. The occlusal plane can be easily affected by tooth eruption and dental development as well as by orthodontic treatment (Richardson, 1982; Frank, 1983; Sherman et al., 1988). This can profoundly influence the Wits appraisal. Furthermore , accurate identification of the occlusal plane is not always easy or accurately reproducible ( Rushton et al. , 1991 ; Haynes and Chau, 1995 ), especially in mixed dentition patients or patients with open bite, canted occlusal plane, multiple impactions, missing teeth, skeletal asymmetries, or steep curve of Spee. Therefore, a new Cephalometric measurement named the W angle was introduced to assess the sagittal relationship between maxilla and mandible with accuracy and reproducibility.This angle uses three skeletal landmarks — point S, point M, and point G — to measure an angle that indicates the severity and the type of skeletal dysplasia in the sagittal dimension.
Objectives
To understand that soft tissue drape could be misleading in diagnosis and treatment plan of malocclusion, so to perform the necessary cephalometric diagnostic hard and soft tissue analysis.6
To understand the significance of certain cephalometric parameters that determine the malocclusion as skeletal class I like W angle7 along with WITS5 appraisal ANB angle.8
To understand the correlation of SNA, SNB, ANB, W ANGLE, with class I class II and class III patients. To study soft tissue facial profile specifically upper lip thickness using soft tissue analysis and understanding the importance of three valuable measurements used in the study.
To analyse the role of KEY RIDGE9 in determining Angle’s class I and the underlying skeletal malocclusion.
Material and Methods
Several reference Angle’s are prescribed in the literature and have been used in previous studies for evaluating skeletal relationship and lip thickness and soft tissue profile. These include SNA angle, SNB angle, ANB angle, WITS appraisal5, W angle and KEY RIDGE9
All of these Angle’s are related to facial growth; therefore, they could be used as reference to measure skeletal relationship between maxilla and mandible,10 Lateral cephalograms were obtained in NHP (Natural head position) position of size (20×25cm) FUJIFILM and lateral cephalograms were obtained on films and some were obtained and retained as soft copies. Manual tracing of 100 lateral cephalogram was done manually using tracing papers with the help of tracing backlight box .Tracing was done with lead pencil point of 0..3mm After tracing manually various cephalometric landmark were marked, measurement were done using the help of geometric box protractor ,divider ,pointer, set square, lead pencil (0.3 mm HB) & geometry box. Lacquered polyester single matte tracing papers from CITIZEN of 50 micron thickness, tracing backlight box.
All cephalograms that were taken in natural head position (NHP).11 The natural head position was used to establish a reliable and reproducible reference line from which the linear measurements could be calculated. Patients radiographs were taken and traced with pencil on a tracing paper .The landmarks were marked and the parameters were measured manually with the help of tools of the geometry box and the values were noted measured and written on the individual proforma chart. This manual tracing on x ray films was done for 100 cephalograms
Using tracing backlight box with uniform lighting and same pencil for all 100 tracings.
A) Skeletal relationship
The following values were measured and entered in a tabular form in the proforma
The following parameters for the evaluation of SKELETAL RELATIONSHIP were traced and the measurements were recorded and the inferences were obtained on the proforma chart.
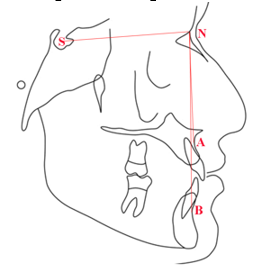
SNA angle, SNB angle and ANB angle8
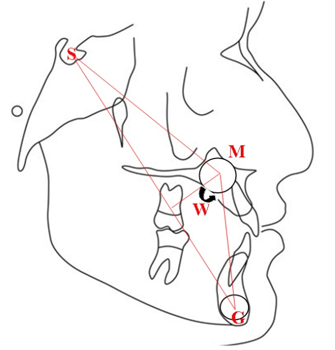
W angle7
It’s a new angle formed by using three skeletal landmarks point S – midpoint of sella turcica ,point M – midpoint of premaxilla ,point G centre of largest circle that is tangent to internal inferior, anterior and posterior surfaces of mandibular symphysis, the line segment SN ,MG and SG are connected and a line from point M perpendicular to SG line is drawn and the angle between the perpendicular line from M to SG and line MG is W angle .This angle is used for assessing the intermaxillary skeletal discrepancy in the sagittal plane.
B) Soft tissue analysis of following parameters for evaluating upper lip thickness were done and measurements and inference were recorded on proforma sheets comparing them to the STCA values given by Arnett for white population
1) Upper lip thickness (the horizontal distance between Labrale superius (Ls)and vermillion border of lip)

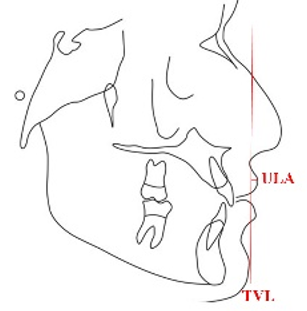
2) Projection of upper lip to TVL (True Vertical Line) or upper lip anterior (ULA)11 drawing of true vertical line: This is a line drawn through subnasale parallel to the chain representing the true vertical and perpendicular to the NHP.The horizontal distance from TVL to the most anterior portion of lip is measured.
Distance from TVL to anterior part of lip is measured.
Figure 5
Schematic representation of measurement of projection of upper lip to true vertical line or upper lip anterior (ULA)
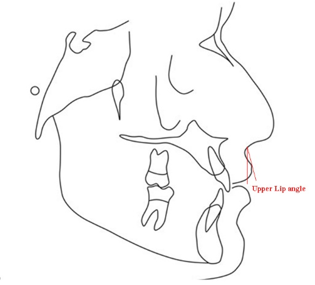
3) Upper Lip Angle (angle formed by segment labial superioris to pogonion and labial superioris to vermillion border of lip)12
The obtained values were also compared with the values depicted by studies on Indian population out of which the parameter of upper lip thickness (ULT)
C) Tracing of key ridge9
Following landmarks are selected
Long axis of molar (mesiobuccal cusp to mesiobuccal root tip)
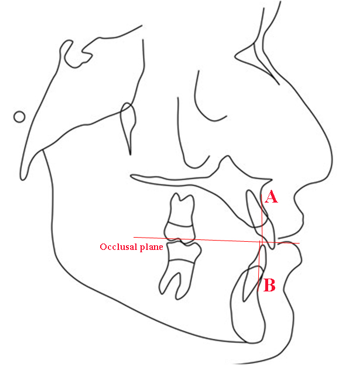
Occlusal plane (a line passing through the intercuspation of molars ,premolars and bisecting the overbite)
Point KR (representing key ridge of infrazygomatic crest)
Point KO
Line KO
Nasion
Point A
Point B
Figure 7
Schematic measurement of distance of key ridgeto mesiobuccal root of permanent maxillary first molar
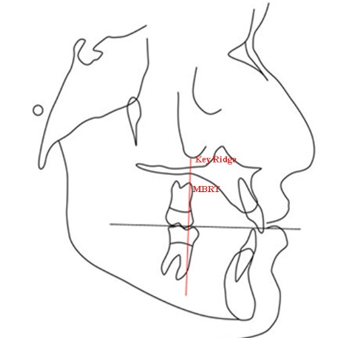
Horizontal distance of key ridge from the mesiobuccal cusp tip (MBCT) and mesiobuccal root tip (MBRT) of maxillary first molar was measured and according to values obtained, it was confirmed that the malocclusion was Angle’s class I malocclusion5
Result
The study parameter measurement and standard deviation by manual method was given in Table 1. The measurement of parmaters included in the study were as follows:
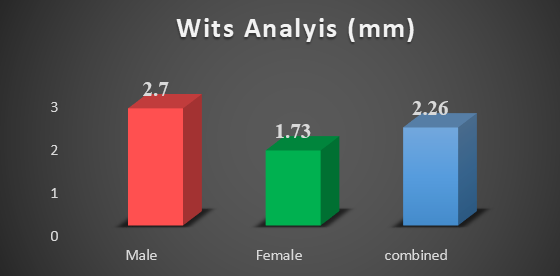
SNA = 83.45°±4.23°, SNB = 79.34°±4.48°, ANB = 4.05°±2.40°, Wits Analysis = 2.26±2.25
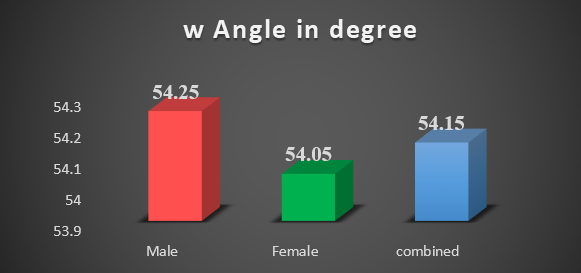
W angle = 54.15±3.09, Upper Lip Thickness = 10.39±2.02, Projection form = 4.39±1.85, Upper Lip Angle = 11.89±7.63 and Key ridge = 6.65±2.63.
Table 1
Study parameter measured byclinical methods
The parameters were compared between males and females and it was documented in Table 2. The measurement SNA among male was 82.35°±4.35° and female was 84.55°±4.11°. There were significant difference between the values of SNA between males and females.
Table 2
Comparison between males and females
The measurement Wits analysis among male was 2.70±2.72 and female was 1.73±2.09.There were significant difference between the values of SNA between males and females. (Figure 8)
There were significant difference between the values of W angle between males and females. (Figure 9)
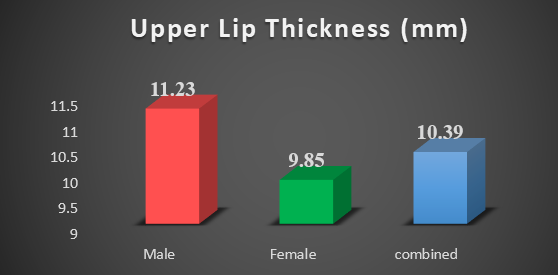
The measurement Upper Lip Thickness among male was 11.23±2.01mm and female was 9.85±2.01mm.There were significant difference between the values of W angle between males and females. (Figure 10)
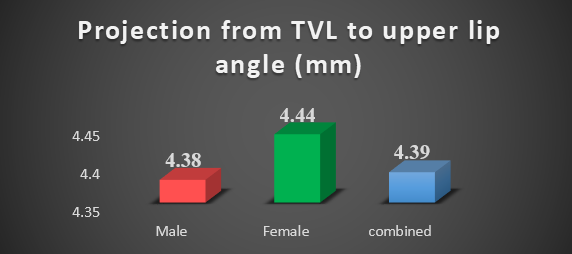
The measurement projection from TVL to upper lip angle also known as upper lip anterior among male was 4.39±1.81 mm and female was 4.44±1.85mm.There were significant difference between the values of W angle between males and females. (Figure 11)
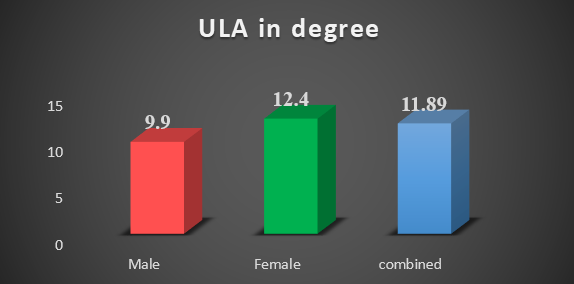
The measurement of Lip angle among male was 9.9°±7.37° and female was 12.40°±7.65 °.There were significant difference between the values of W angle between males and females. (Figure 12)
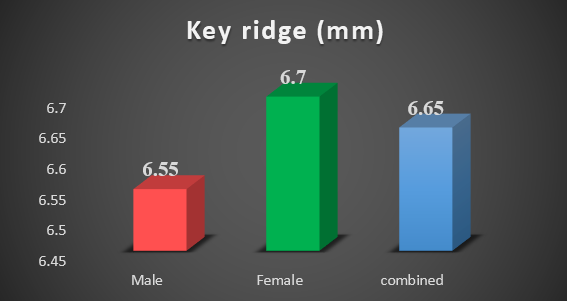
The measurement Key ridge among male was 6.55±2.54 and female was 6.70±2.73.There were non-significant difference between the values of W angle between males and females. (Figure 13)
The correlation between Wits analysis and ANB was done. The test result shows that there were moderate Positive correlation between the two variables with correlation coefficient 0.50. (Table 3).
Table 3
Pearson correlation between anb and wits analysis
|
Variable 1 |
Variable 2 |
Correlation Coefficient |
P value |
|
ANB angle |
Wits Analysis |
0.50 |
0.001* |
The upper lip thickness shows strong negative correlation with W angle while the Key ridge shows strong positive correlation with W angle but the correlation are not significant. While the Upper lip Anterior ad Lip angle shows moderate positive correlation with W angle. The upper lip thickness can be used as predictor in class I relationship as it is strongly correlated with W angle (Table 4)
Table 4
Correlation of upper lip thickness, projection from tvl to ulanterior, upper lip angle, w angle and key ridge
Discussion
For a treatment resolution of a given malocclusion, it might be easy for any orthodontist to believe that adhering to certain arbitrary standards will automatically lead to desirable treatment result. But a wise approach is to treat the real objectives as suggested by Jackson’s triad – esthetic stability and function.13 Lip thickness and lip posture are very closely associated with all these objectives .Normally the dentoskeletal and soft tissue standards serve as guides in treating orthodontic patients,14 however the facts that variation in the lip thickness and lip posture of every individual and variation in the dentoskeletal pattern of each individual,15 This approach seems to be incomplete and its validity needs to be questioned. Therefore this study is trying to formulate the need of a better approach where accurate anterioposterior skeletal relationships and diagnosis is generated through cephalometric treatment planning where STCA is used as a guide and correlated with the accurate skeletal discrepancy.
As per Arnett et al.12 the CTP states that the incisor and the maxilla should be moved forward when the upper lip is thick and upper lip angle is upright .in the present study. As per Arnett thick upper lip coincides with midface retrusion .According to author thick upper lip correlates with retruded maxilla and vice versa. The upper lip angle reflects the position of the upper incisor teeth and the thickness of the soft tissue overlying this teeth. This angle is very important for an orthodontist to make an extraction decision. If upper lip angle is increased it may suggest an extraction approach.My present study shows that the measurement of Upper Lip Thickness among male was 11.23±2.01mm and female was 9.85±2.01mm. But what is important is that cephalogram should be taken in natural head position, seated condyles, and relaxed lip position for an accurate evaluation.seperate values should be followed for male and females and for different races and different regions. The present study focuses on age specific and gender specific values for central Indian population as less study for the same has been done in central India ethnic values and article to be added. Here it is important to state that CTP with the help of STCA is not sufficient to fulfill the aim of orthodontic treatment .The underlying jaw relation which many a time goes unnoticed and only the dental problems are addressed leaving the sagittal skeletal discrepancy untreated. The cephalometric measurement of SNA SNB ANB and wits appraisal have their limitation to be accurate all the time because of their dependence on several factors .this study also uses a new cephalometric measurement that is W angle as suggested by W A Bhad et al.7 (Bhad W, Nayak S, Doshi U. A new approach of assessing sagittal dysplasia: The W angle. Eur J Orthod. 2011;1-5)`. to diagnose the sagittal discrepancy between maxilla and mandible with great accuracy and the measurements are made and compared with the norms as suggested in this article. Hence with the sound knowledge of underlying skeletal malocclusion and CTP we should be able to make better diagnosis and treatment planning for patients. However this is meant to be used along with accurate clinical examination, model analysis or various other suitable diagnostic aids. Serial radiographic measurements obtained from the manual tracing and digital tracing of the values of the landmarks like SNA angle, SNB angle , ANB angle, WITS APPRAISAL,W angle, upper lip anterior, protrusion of lip to TVL, upper lip angle determines that there is a correlation between the soft tissue and hard tissue measurements.
Many system have been developed to classify malocclusion. Kingsley, Angle, Case, Dewey Anderson, Hellman, Bennet, Simon, Ackerman and profitt etc.1, 2, 3 The classification given by E. H Angle is universally most accepted and was given in 1889, based on the position of maxillary first molar in the craniofacial anatomy.1 Angle gave his classification of malocclusion assuming that the position of maxillary first molar is unchangeable and it lies on the key ridge. So anatomically maxillary first molar rest on the broad buttress of bone of the cranial base. Key ridge was given by Atkinson on 1923.16 The key ridge was first shown by Sicher and Drubrul as a pillar of trajectories in the craniofacial anatomy. The strong key ridge of bone projects downward from the anterior end of the zygomatic process and normally extends over the mesiobuccal roots of the upper permanent molar.17, 18 The position of key ridge never changes and its position is same irrespective to age, race and what happens to tooth or alveolar bone.19 This study points out that key ridge plays an important role in determining Angle’s class I and underlying skeletal malocclusion.
Conclusion
It has been found by this study that tissue drape is an important parameter in diagnosis and treatment planning.
Upper lip thickness is a major decipherer of orthodontic treatment plan .Soft tissue facial profile and upper lip thickness should be decoded and soft tissue analysis using STCA are mandatory for good diagnosis and treatment planning
Cephalometric parameters that determine the malocclusion as skeletal class I, class II and class III i.e. W angle WITS appraisal, and ANB angle were pertinent and W angle was found adequately reliable.
This study specifies that variation in lip thickness and lip posture of every individual and the variations in the dentoskeletal pattern of each individual, make it essential to generate the diagnosis through cephalometric treatment planning (CTP) where STCA is used as a guide and correlated with accurate underlying skeletal discrepancy .More studies on this subject can be conducted in future in different parts of the world, and that will further validate the study.