Introduction
In this modernizing era, People now tends to experiment things that necessitate professional aid on their own. This originated with semi-skilled or non-skilled works and it soon evolved to works requiring professional skills, this approach is referred as “Do-it-Yourself (DIY)"
Commercial tele-dentistry has aggressively promoted DIY orthodontics, DIY aligners, and DIY braces through non-dental professionals, and as a result, the patient perspective, particularly in orthodontics, has undergone a significant transformation. DIY orthodontics began with household items like rubber bands, dental floss, and paper clips being used to move teeth and eventually advanced to 3D printing and aligner technology. Dental care is delivered via digital information exchanged through tele- communication dentistry rather than through face-to-face interactions with a dentist or orthodontist.
DIY treatment having the advantage of being a fraction of the expense of traditional practice-based orthodontics, sometimes reported as 60%-70% less expensive, as well as the convenience of not having to attend and travel for visits.1 Nevertheless, a number of international specialty dentistry organisations have voiced their worries over issues pertaining to the assessment of suitability, consent, safety, regulation, and scope of practise.
The majority of DIY aligner marketing, advertising, information exchange, and consent processes take place online. Customers typically use product websites to learn more before making a purchase decision. A literature review revealed limited literature regarding the information available and quality of treatment rendered and its outcome on DIY-orthodontic company websites. The present study is aimed to fill that knowledge gap by conducting the survey on esthetical outcomes of results posted by DIY aligner companies in their marketing websites.
Aim and Objective
The study's main goal was to evaluate the cosmetic results of treatment provided by DIY aligners companies and professional orthodontist by collecting 15 set of pre and post photographs of rendered treatment posted in their website for marketing and the secondary aim was to access the view on DIY aligner companies among general dental practitioners and orthodontists.
Materials and Methods
Methodology
Search terms like DIY aligner companies in India, Do it yourself aligners were entered in search engines, the popping up aligner companies websites were logged in to assess 15 random sets of pre and post orthodontic treatment photographs posted in their website for marketing (group A) were chose, Similarly 15 random sets of pre and post orthodontic treatment photographs posted by professional orthodontist in social media (group B) were chose. These photographs were jumbled up to form an online survey via Google form and sent to 110 orthodontist and 110 general dentists to assess the esthetic perception with the help of Likert’s scale. Descriptive statistics was obtained from google form. The chi square test was used to investigate significant difference between groups. The whole set of data was entered into MS Excel prior to statistical analysis (P-value 0.05 was regarded as statistically significant). To better understand the statistically significant difference, all findings are presented in tabular and graphical formats.
Ethical approval was not necessary as this investigation assessed publicly available information only
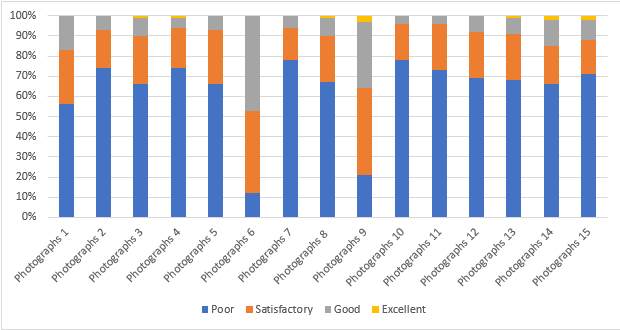
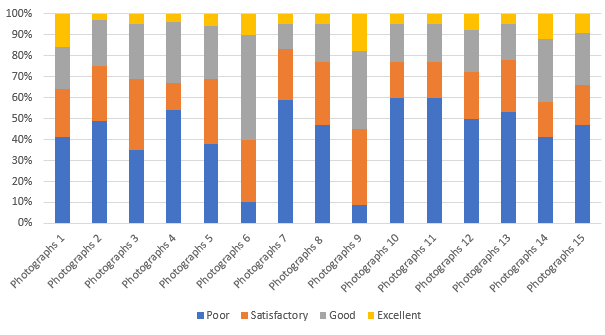
Table 1
Likert’s scale response percentage of esthetical satisfaction in Group A
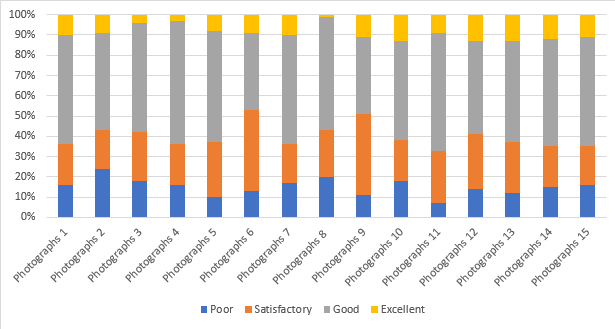
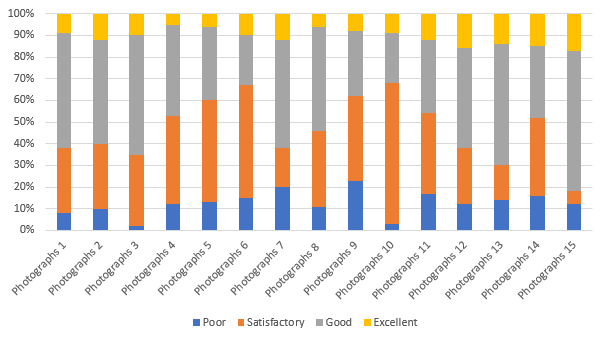
Table 2
Likert’s scale response percentage of esthetical satisfaction in Group B
Results
Responses of esthetical satisfaction of treatment rendered by DIY aligner companies (group A) and professional orthodontist (group B) are tabulated based on Likert scale percentage among orthodontist and general dentist subgroups in Table 1 and Table 2 respectively.
Esthetic outcomes were significantly better in orthodontic treatment rendered by professionals as compared to DIY aligner companies (p<0.005). Inter comparison between orthodontist and other dental surgeon is non-significant as both Dentist and orthodontist are in favour of treatment rendered by professionals as compared to DIY aligner companies.
Discussion
Customers are constantly looking for the ideal smile at an affordable price, which has led to an increase in the number of companies offering DIY braces. More clients are being convinced to try DIY orthodontics rather than getting treatment from a conventional orthodontist or dentist as a result of the COVID-19 pandemic's impact on access to orthodontic appointments.
In recent research by Bous et al.2 in 2021 containing 1141 respondents to a questionnaire, consumers choose DIY orthodontics primarily for convenience and cost, with 26.6% of them more likely to do so as a result of the COVID-19 pandemic. Another study by Okuda et al.3 2021 confirmed the primary factors behind DIY orthodontics being cost and convenience.
Despite the fact that it at first sounds alluring, simple, and economical, it ultimately results in serious, irreparable harm to the tooth, gums, and supporting bone structure, leaving the dentition in a damaged state. The information that can be seen on the websites of these companies is typically unregulated and devoid of any standards to validate the treatment claims. The danger of self-impressions is another issue that the general people is ignorant of. There have been numerous reports of impression material becoming loose and suffocating. An additional worry is that any appliances or aligners created using these shoddy impressions may not fit well and cause additional harm to the teeth and gums.
Prior to initiating any treatment, a clinical evaluation is necessary to address any oral health problems that may be present. This also enables the physician to decide whether the proposed orthodontic therapy is secure, appropriate, and in the patient's best interests. Additionally, patients can consider the benefits and drawbacks of all available options during clinical contact, provide valid, informed consent, and feel sure that a suggested course of therapy will likely satisfy their needs and expectations. The DIY providers have no opportunity to evaluate and discuss such difficulties, complex treatment requirements, or the cosmetic effects that straightening teeth will or won't have on their occlusion or facial profile. This is a rigorous limitation, and the permission process frequently entails it i.e. in the absence of informed choice, valid consent cannot be achieved.
According to Wexler et al.4 (2020), clients in the United States who wished to lodge a complaint and gain a refund from particular businesses had to sign a non-disclosure agreement to prohibit them from posting negative reviews on social media or websites. Given this, it could be challenging to gather reliable data on consumer experience on social media platforms, which are an important instrument for these companies' marketing strategies.
In a study by Okuda et al.3 2021 discovered that when household income, age, and education increased, people were more inclined to pick DIY aligners, which differs from conventional dentist perceptions and should assist societies prioritise public education. The American Association of Orthodontists (AAO) reported the Smile Direct Club's Service as "illegal and poses medical concerns" to the authorities in 36 US states in 2019. By submitting a citizen petition to the Food and Drug Administration in 2019, the American Dental Association expressed its strong opposition to the trend of at-home clear aligner therapy and sought to include it in the category of DIY dentistry, which is quickly growing in popularity (FDA). The British Orthodontic Society, along with 31 other professional dentistry and orthodontic societies from 25 other countries, established the European Federation of Orthodontic Specialists Associations in November 2021 and issued a common declaration outlining the fundamental prerequisites for any orthodontic treatment. The Indian Orthodontic Society (IOS) has acted strongly to combat DIY aligners and dispel the widespread myth that a qualified orthodontist is not necessarily necessary. In November 2021, the IOS sent a representation to the Dental Council of India (DCI) outlining the numerous Code of Ethics violations committed by DIY-aligner businesses while providing in-home services. The recommendation emphasises the requirement for the highest standard of care based on appropriate evidence-based diagnostic and treatment planning, biological waste management and sterilisation processes, and ethical business practices and marketing.4, 5
Remote-orthodontic technology, tele-dentistry can be beneficial when utilised properly and appropriately by dentists to enhance traditional orthodontics, such as with Align Technology, Dental Monitoring or Smile Tracker apps. This digital technology is starting to be used by orthodontic specialists themselves to remotely monitor clear aligners. These developments are beneficial for modernising orthodontist-supervision but inappropriate usage by non-professionals may result in hazards.
Conclusion
This current study demonstrates unambiguously that the treatment provided by DIY Aligner companies were poor. Orthodontists are the essence of orthodontic treatment, not aligners. A flawed diagnosis and an inadequate treatment plan may result from the absence of a full, in-person pretreatment examination by a licensed orthodontist and data gathering by a skilled professional. A tele dentistry business might mistakenly identify a person with a malocclusion that cannot be effectively treated with these aligner systems as a candidate. People who believed they could receive orthodontic treatment at a significantly reduced cost without the direct supervision of a trained orthodontist, discovered after undergoing aligner therapy that correcting their malocclusion was not reasonably possible with the DIY clear aligner system. The general public should be informed that correcting the negative effects of poorly planned or poorly fitted clear aligners may ultimately cost them extra money.
Thus, Orthodontists need to augment and aggressively increase public awareness regarding the ill effects of DIY aligners.