Introduction
Distalization is a well-documented technique employed to increase arch length. It is a conservative method of gaining space without sacrificing the dental units.1 The process of molar distalization has been in practice for over a century and has evolved leaps and bound ever since. Numerous methods have been proposed over the years using both intra-oral and extra-oral appliances.2, 3
Traditionally, headgears were used as an extra-oral method of molar distalization. Though effective, headgears are highly dependent on patient compliance and therefore, intra-oral fixed appliances gained popularity. One such appliance that is widely used even today is known as the Pendulum appliance introduced by Hilgers in the year 1992.4, 5 Anchorage planning and appliance design are the keys to a successful treatment outcome using the appliance. Certain adverse effects such as distal tipping of molars, an undesired increase in lower anterior facial height and mandibular clockwise rotation have been reported in literature.6
Temporary anchorage devices (TADs) have revolutionised the way anchorage is managed in contemporary orthodontics. TADs have been utilised in distalization as well and literature has suggested effective distalization with minimal tipping using the same. However, recent systematic reviews suggest that effective distalization can be achieved with both conventional and TAD mechanics without much clinically significant differences.7 TADs have certain disadvantages like screw failures, approximation to root surfaces and associated pain.8 Thus, TADs may be specifically employed in critical anchorage cases.
The present article describes two such cases which have been effectively treated using the conventional pendulum appliance with TADs along with aesthetically pleasing outcomes.
Case 1
A 11 years old female patient reported to a tertiary care dental centre with the chief complaint of Irregular upper front teeth. The patient started noticing the problem since the eruption of permanent teeth and desired correction of the same. The medical and dental history of the patient was non-contributory. The growth history revealed that the patient had not achieved menarche.
Clinical examination
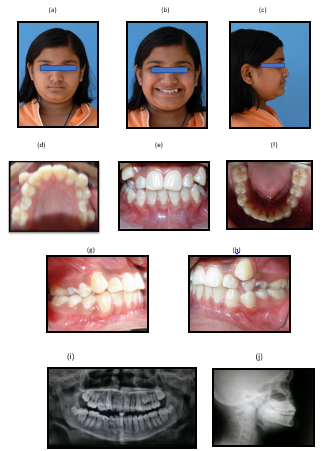
Extra Oral: Patient’s face was proportional in the horizontal fifths and vertical thirds. The patient had a non-consonant smile arc and wide buccal corridors. The profile was straight with a deep mentolabial sulcus and an obtuse chin-throat angle. [Figure 1 (a-c).
Intra Oral: Intra oral examination revealed severe crowding in the upper arch, rotated 15 and 25, blocked out 13, labially displaced 23, upper midline deviated to right by 2 mm, mild lower arch crowding end on molar relation and a non-specific canine relation. (Figure 1 d-h).
Radiographic assessment
Orthopantamogram: revealed permanent dentition with the 3rd molars in various stages of eruption. No abnormality was detected. (Figure 1 i)
Lateral Cephalogram: revealed mild class III skeletal bases with an average growth pattern. Proclination of the maxillary anteriors and a normal lower anterior facial height. Adequate molar-Ptv value (Table 1 & Figure 1 j).
Problem list
Based on the clinical examination and radiographic assessment the following problem list was formulated:
Treatment progress
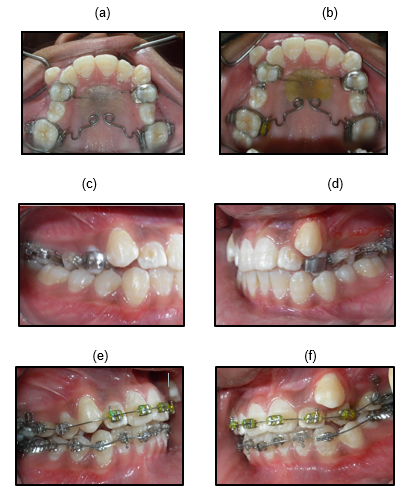
Molar distalization using the pendulum appliance [Figure 2 (a-b)]. Distalization was achieved in four months and E chains were employed for derotation of premolars [Figure 2 (c & d)]
Bonding was done using 0.022” MBT pre-adjusted edgewise appliance and levelling and alignment was carried out [Figure 2 (e & f)].

Case 2
A 19 years old female patient reported to a tertiary care dental centre with the chief complaint of Irregular upper front teeth. The medical and dental history of the patient was non-contributory.
Clinical examination
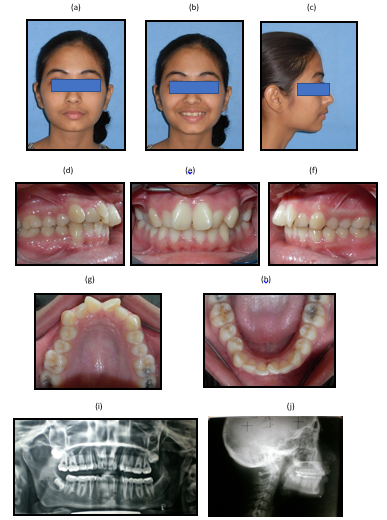
Extra Oral: Patient’s face was proportional in the horizontal fifths and vertical thirds. The patient had a non-consonant smile arc and wide buccal corridors. The profile was convex with an increased nasolabial angle. [Figure 4 (a-c)]
Intra Oral: Intra oral examination revealed moderate crowding in the maxillary arch, mild crowding in the mandibular arch and end on molar and canine relations on the left and class II on the right side. (Figure 4 (d-h)].

Radiographic assessment
1. Orthopantamogram: revealed permanent dentition with the 3rd molars in various stages of eruption. Missing 38. No other abnormality was detected.[Figure 4 i].
2.Lateral Cephalogram: revealed class I skeletal bases with an average growth pattern. Proclination of the maxillary anteriors and a normal lower anterior facial height. (Table 3 &Figure 4 j)
Problem list
Based on the clinical examination and radiographic assessment the following problem list was formulated:
Treatment progress
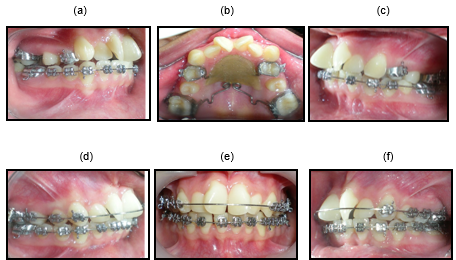
Bonding was done using 0.022” MBT pre-adjusted edgewise appliance and levelling and alignment was carried out [Figure 5 d-f].
Conclusion
Distalization is one of the most widely accepted modalities of gaining space. Case selection is vital in such cases as distalization may affect the lower anterior facial height adversely. A thorough clinical and radiographic assessment form the basic tenets of a successful treatment outcome. The intra-oral appliances are used popularly as these do not require patient compliance. With the recent advances in technology numerous distalization appliances have been introduced over the years.9 However, the conventional appliances still remain as effective when utilized in the correct way and modified as per the specific requirement of a particular case.