Introduction
Orthodontic treatment has the ability to move the teeth precisely and in a planned manner in all three planes of space within the alveolar bone. Simultaneously, it adversely affects the surrounding structure like clinical attachment loss, subgingival microbial changes, root resorption, enamel demineralization, and discoloration.1, 2 Among these adverse effects of orthodontic treatment, enamel subsurface demineralization or white spot lesions (WSLs) are commonly seen in orthodontic patients with a 45.8% of incidence rate and 68.4% of prevalence.3, 4 Majority of WSLs are associated with the gingival area of upper lateral incisors, lower canines, and premolars.5 Younger patients have more chances to develop the lesion during orthodontic treatment as compared with adults.6 Self-cleansing mechanisms of oral cavity impeded by multibracket system of orthodontic therapy result in accumulation of plaque and lowering of PH, that ultimately leads to enamel demineralization.7, 8 Increased incidence of enamel demineralization in fixed orthodontics is already proven with various studies.9, 10, 11
Clear aligner (CA) therapy is one of the recent advances in orthodontics and becoming popular with time due to the increase in the number of young and adult patients looking for a more aesthetic and comfortable alternative to fixed appliances (FAs). The effectiveness of CA therapy is already proven with different studies and systematic reviews.6, 12, 13 Recent studies claim that the incidence of WSLs is decreased in aligner therapy.14 Purpose of this systematic review was to assess the enamel demineralization in clear aligner treatment compared with conventional multibracket system. The null hypothesis was assumed that there is no difference regarding incidence and characteristics of enamel demineralization between fixed multibracket system and clear aligner therapy.
Materials and Methods
Protocol and registration
Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) guidelines (http://www.prisma-statement.org/)15 and the Cochrane Handbook for Systematic Reviews of Intervention (https://www.cochrane-handbook.org/)16 were used for conduction and reporting and analysis. Systematic review was registered in PROSPERO and the registration number was CRD42021261169.
Eligibility criteria
Eligibility criteria of analysis has been set according to the PICOS format described as:
Participants
Mild to moderate class I malocclusion (<5 mm of crowding) with non-extraction treatment plan.
Comparison
Fixed orthodontic treatment was performed in mild class I malocclusion (crowding < 5mm, with non-extraction treatment plan) as a control group.
Outcome
The incidence rate of WSLs, depth of enamel demineralization, and surface area of developed lesions.
Study design
Randomized controlled clinical trials, prospective studies, and in-vivo studies were included.
Exclusion criteria
Subjects who have not undergone any orthodontic therapy, patients with severe malocclusion and skeletal discrepancies, patients with craniofacial syndromes, malocclusion treated with myofunctional and orthopedic appliances, patients underwent either CA therapy or FA therapy who have compared WSLs before and after the treatment, Retrospective studies, case series, case reports, literature reviews, in-vitro studies, observational studies, authors' opinion, letters to the editor, and engineering articles were excluded. Focused question of the study was “Do clear aligner therapy show a lesser incidence rate of WSLs compared to fixed orthodontic treatment?”
Search Methodology
A comprehensive search was done from January 2020 to September 2021 with no publication year limits by two independent reviewers (VS and DS). Following electronic databases were searched for published studies- PubMed (https://pubmed.ncbi.nlm.nih.gov/), Cochrane Collaboration Oral Health group database of clinical trials (https://www.cochrane.org/), Web of Science (https://mjl.clarivate.com/search-results), Science Direct (https://www.sciencedirect.com/), Scopus (http://www.scopus.com/). In addition to this, a manual search of the references mentioned in the included studies and grey literature was done.
In-vivo randomized controlled clinical trials and prospective studies were included in this study to check and compare the incidence rate of newly developed WSLs in patients who underwent orthodontic treatment with either CA compared with FA therapy.
Following keywords were used during literature search 1. White spot lesions 2. Clear aligners 3. Traditional braces 4. Fixed orthodontic treatment 5. Enamel demineralization 6. Initial carious lesions 7. Subsurface demineralization 8. Invisalign.
Boolean operators OR and were used in combination with these keywords to search published studies.
Combinations of keywords were used in electronic databases during literature search were “Clear aligners AND White spot lesions”, “Clear aligners AND Enamel demineralization”, “Clear aligners AND White spot lesions OR Enamel demineralization”, “Clear aligners AND Traditional braces AND White spot lesions”, “Invisalign AND White spot lesion AND Traditional braces”, “Fixed orthodontic treatment OR Invisalign AND White spot lesions” and “Fixed orthodontic treatment AND Subsurface demineralization OR Initial carious lesions”.
Data collection
The data were extracted by two independent reviewers (PP and TP) from all the included studies and filled them into predetermined forms. From each study, following data were obtained – study design, publication year, country, sample size, sample gender, sample age, intervention, follow-up period, analysis, and outcomes.
Data analysis
Studies will be considered for meta-analysis, if presented with sufficient homogenous data otherwise qualitative analysis would have been undertaken. Incidence of white spot lesion after both the treatment procedures was planned to assessed by the software review manager 5.03 (RevMan, Nordic Cochrane Centre, Copenhagen, Denmark). Bivariant differential mean statistic was planned for an intergroup estimate with 95% confidence interval to measure outcome mean. Random effect model with Cochran–Mantel–Haenszel statistics17 was used. To identify study heterogeneity I2 test statistics were applied and P value <0.05 was considered significant statistically.
Risk of bias and quality of evidence assessment
Two independent reviewers (DS and RS) assessed the bias of the included studies and any disagreements were solved by discussion. The risk of bias of the included randomized clinical controlled trials was evaluated using the Cochrane risk of bias assessment tool and a plot was generated using Rob 2.0 Cluster (https://www.riskofbias.info/welcome/rob-2-0-tool).18 The traffic signal plot consisted of five domains (D1 to D5) indicating selection, detection, attrition, reporting, and other bias. ROBINS-1 (https://www.riskofbias.info/welcome/home/current-version-of-robins-i)19 was used for risk of bias assessment of the included non-randomized prospective study assessed by seven different domains. Overall bias and bias of each domain was decided to be low (low for all key domains), moderate (moderate risk in at least one domain), serious (serious risk in at least one domain), critical (critical risk in at least one domain) or no information. Along with this, GRADE tool (https://www.gradepro.org/) was also used to evaluate the quality of evidence for all the included studies.
ResultsStudy selection
The literature search yielded a total of 479 studies through search in electronic databases (PubMed- 218, Cochrane central- 145, ScienceDirect- 51, Web of Science- 65). Among all the studies, 130 duplicate records were removed.345 studies were removed after screening title and abstracts. Table 4 studies were included for full-text reading; one study was excluded due to other reasons.14, 20, 21, 22 Among three studies, two randomized controlled clinical trials and one prospective study were included for qualitative and quantitative analysis.20, 21, 22 The study selection procedure was done by two independent reviewers (VS and DS) and any disagreements between the reviewers were solved by discussion. The study selection procedure has been shown in Figure 1 a.
Figure 1
a) PRISMA flow diagram shows selection process of eligible studies; b) Traffic signal plot of assessment of RCCT with the Cochrane risk of bias tool; c) Traffic signal plot of risk of bias assessment in prospective study; d) GRADE tool for the assessment of quality of evidence.
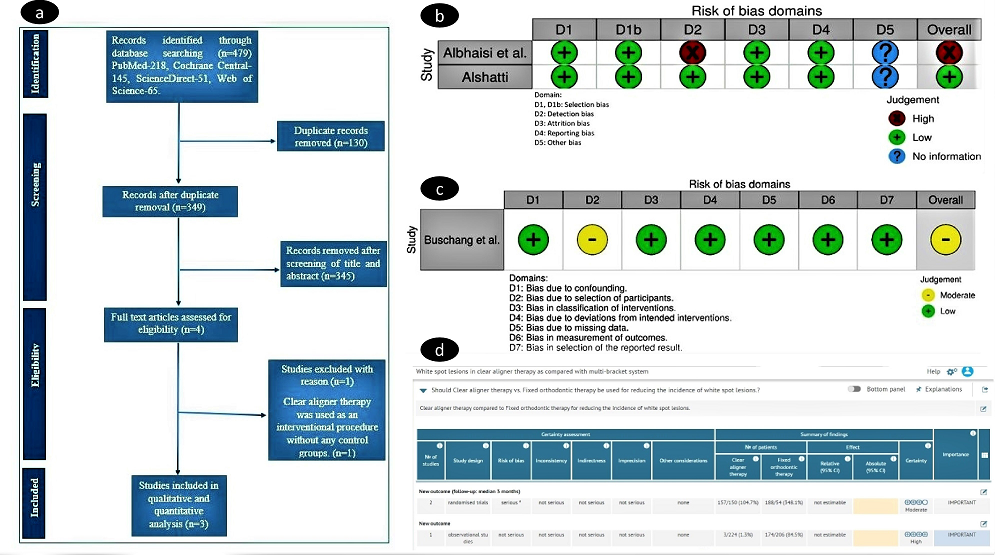
Table 1
Characteristics of included studies
|
Studies |
Number of subjects |
Age group and Gender |
Treatment duration and Follow-up |
Variables |
Outcome |
|
Albhaisi et al., 2020 20 |
49 subjects taken, 42 complete |
21.25±3 years for both CA and |
Duration of the treatment was not |
Primary outcome variable; |
Post-treatment mean fluorescence loss was higher in |
|
|
d the study |
FA group. |
mentioned |
Newly developed white spot |
FA group. |
|
|
19 (CA group) |
39 females and 10 males. |
Outcome variables were measured during treatment (3 months). |
Lesions |
Newly developed white spot lesions were found more in FA group. |
|
|
23 (FA group) |
|
|
Secondary outcome variables; 1. Mean amount of fluorescence loss. 2. Deepest point in the lesion. 3. Lesion area in pixel format. 4. Plaque surface area |
Value of deepest point in lesion was significantly higher in FA group. Lesion area was significantly higher in CA group. FA group exhibit significantly more plaque accumulation than CA group. |
|
Buschang et al., 2020 22 |
CA group-244 subjects |
30.4±14 years; CA group |
CA therapy- 1.5±0.9 years |
Change in pre-treatment and post-treatment oral hygiene status |
Oral hygiene was better in patients with removable aligners. |
|
|
FA group-206 subjects |
29.2±11.5 years; FA group |
FA treatment- 2.5±1.3 years |
Incidence of white spot lesions |
Less incidence of developing white spot lesion in aligner group |
|
|
|
No gender description. |
No follow-up period was mentioned. |
|
|
|
Alshatti,2017 21 |
24 subjects (CA therapy) |
17-24 years age group |
16.83±5.11 months (CA therapy) |
Incidence of white spot lesion |
Incidence of white spot lesion in clear aligner group was found low as compare to conventional and self-ligating bracket groups. |
|
|
16 subjects, self-ligating brackets (FA) |
No gender description. |
17.40±6.28 (self-ligating brackets- FA) |
Surface area or severity of white spot lesion |
Surface area of white spot lesion in clear aligner group was more but less severe in nature. |
|
|
19 subjects, conventional brackets subjects (FA) |
|
19.52±4.40 (conventional brackets- FA) Outcome was |
Correlation between gingival, plaque and bleeding indices and |
Gingival, plaque and bleeding indices values for clear aligner group were always lower than fixed appliance group. |
|
|
|
|
Measured after 9 and 18 months of treatment. |
White spot lesions. |
|
Table 2
Characteristics of included studies (Extended)
|
Study |
Study design |
Definition of WSLs or Enamel demineralization |
Method used |
Intervention |
Additional information |
|
Albhaisi et al., 2020 20 |
Randomised controlled clinical trial |
Not mentioned |
Quantitative light-induced fluorescence (QLF) images |
Group-1 received CA treatment (Eon Aligner) |
Priori sample calculation; yes |
|
|
|
|
|
Group-2 treated with FA (Gemini Metal Bracket, 3M Unitek) |
Accuracy of measurements;yes |
|
|
|
|
|
|
Baseline comparability; yes |
|
Buschang et al., 2020 22 |
Prospective study |
Not mentioned |
Digital photographs and specific criteria to evaluate measurements |
One group treated with CA therapy and another treated with FOA treatment |
Priori sample calculation; yes |
|
|
|
|
|
|
Accuracy of measurements;y Baseline comparability; yes |
|
Alshatti, 2017 21 |
Randomized controlled clinical trial |
Not mentioned |
Digital photographs and indices for specific measurements |
Group-1 received CA therapy (Invisalign, Align technology, Santa Clara Califo rnia) |
Priori sample calculation; yes Accuracy of measurements; yes Baseline comparability; yes |
|
|
|
|
|
Group-2 treated with self-ligating brackets (CarriereSelf- Ligating Bracket, Carlsbad, CA) |
|
|
|
|
|
|
Group-3 received conventional pre-adjusted edgewise brackets |
|
Table 3
Assessment of RCCT with the cochrane risk of bias tool
|
Study |
Random sequence generation |
Allocation concealment |
Blinding of outcome assessment |
Incomplete outcome data |
Selective reporting |
Other bias |
Overall risk of bias |
|
Albhaisi et al.20 |
Low |
Low |
High |
Low |
Low |
No information |
High |
|
Alshatti 21 |
Low |
Low |
Low |
Low |
Low |
No information |
Low |
Table 4
Risk of bias assessment with ROBINS-I tool in prospective study
|
Study |
Bias due to confounding |
Bias in selection of participants into study |
Bias in classification of intervention |
Bias due to deviation from intended intervention |
Bias due to missing data |
Bias in measurement of outcome |
Bias in selection of the reported result |
Overall |
|
Buschang et al. 22 |
Low |
Moderate |
Low |
Low |
Low |
Low |
Low |
Moderate |
Characteristics of the included studies
Characteristics of the included studies are presented in Table 1, Table 2.
Total three included studies in this systematic review were conducted in three different regions (Jordon, Texas, Connecticut) and published in between 2017 to 2021.20, 21, 22 Total 551 patients who were treated with either clear aligner therapy or fixed orthodontic appliances were identified. The clear aligner group was comprised of 287 patients whereas 264 patients were present in the fixed orthodontic group. In addition, included age group was found 17 years to a maximum age of 44.4 years. Moreover, gender description was provided only in one study, and the minimum follow-up period was assessed immediately after treatment completion to a maximum of 18-month post-treatment.20 QLF and Digital photographs were used as the method of recording the WSLs.21, 22 Furthermore, all the studies have mentioned the method of prior sample calculation, considered inspecting the accuracy measurement, and compared baseline data.
Results of Individual Studies and Qualitative Synthesis
I2 value was calculated 98% in this analysis and the Chi2 value was greater than the degree of freedom, showing a higher amount of heterogeneity in between the studies. In addition, because of the heterogeneity in study design, intervention, follow-up period, and presence of low-quality studies (high risk bias), a quantitative analysis was not conducted. On qualitative analysis, a total of 160 new white spot lesions were developed in the clear aligner group and 362 new white spot lesions were found in the multibracket fixed orthodontic group. All the three included studies mentioned P <0.001; that indicates a significantly lesser number of newly developed lesions in the clear aligner group. According to Albhaisi et al.,20 post-treatment mean fluorescence loss was higher in the FA group that indicate more newly developed white spot lesions in FA group along with the value of deepest point in the lesion was found significantly higher in the same group. Contrast to the above findings lesion area was significantly higher in the CA group. Similarly, Buschang et al.22 concluded that less incidence of developing white spot lesion seen in the aligner group than FA therapy. In addition, according to Alshatti et al;21 Incidence of white spot lesion in clear aligner group was found low as compared to conventional and self-ligating bracket groups along with the surface area of white spot lesion in clear aligner group was more but less severe in nature. Furthermore, it was also concluded by all the three studies that oral hygiene status was poor with FA therapy (more plaque accumulation and gingival bleeding). Moreover, there was no significant difference found regarding age group and gender during evaluation.
Quality of the included studies
The risk of bias assessment of Randomized controlled clinical trials 20, 21 are summarized in (Table 3, Figure 1 b) and for prospective study21 in (Table 4, Figure c). The risk of bias was assessed, in which one trial 20 was evaluated at high risk of bias due to absence of blinding of outcome assessment and another21 was found to have a low risk of bias. Overall moderate risk of bias in the included prospective study was found 22 because of selection of the participants were done on the basis of the recent completion of cases which led to some concerns regarding the quality of the study, and low risk of bias was judged against the other six domains of the ROBINS-1 tool. (Table 4, Figure 1 c) The quality of evidence was assessed using GRADE tool, on the basis of which, moderate result was found in randomized controlled clinical trials 20, 21 and high outcome was found in the prospective study.22. (Figure 1 d)
Discussion
White spot lesions are aesthetically unpleasant if develop on anterior teeth and influence a person’s confidence and smile.23 This review was done in order to evaluate the incidence of white spot lesions in clear aligner and multibracket fixed appliance therapy. The results show significantly less incidence of white spot lesion in clear aligners as compared to the fixed appliances. (p<0.001) It is in agreement with a study conducted by Muhammad Azeem et al.14 in which patients treated with clear aligners but without taking control group. A possible explanation for this low incidence of enamel demineralization in the CA group may attributable to less food lodgement over appliance since patients do not wear the appliance during the meal, favorable maintenance of oral hygiene, and minimum chances of accumulation of microbial flora i.e., streptococcus mutans and lactobacillus over aligner and tooth surface.24 According to another study, shorter treatment duration in aligners therapy may obviate the risk of developing WSLs as compared with FA therapy.25
Although incidence of WSL is low in clear aligner group, included studies show severe heterogeneity. (I2) Limited flow of saliva to the teeth surfaces while using clear aligner and attachments of appliance may interfere with the self-cleansing activity of saliva resulting in enamel demineralization. 26 Only one study assessed mineral loss and depth of the lesion which is more in the fixed appliance group. 20 The size of WSL developed in patients with fixed appliance treatment were small with greater enamel demineralization and lesions in patients with clear aligner therapy were large with lesser demineralization. 20
The wide attachment bonded on the tooth surface in the CA group may be a possible explanation of wide lesion. Age is considered as a risk factor to develop white spot lesions in orthodontic patients, younger patients most of the preadolescent age group reported with increased incidence of white spot lesions. 11 Study performed by Mizrahi 9 concludes that frequencies of white spot lesions are gender independent. However, contrary to this, other27, 28 disagree with a greater male predilection for developing WSLs.
All three studies included in this systematic review provides data of 551 subjects irrespective of their gender and age to assess the incidence of white spot lesions evaluated with various methods like digital photography and quantitative light-induced fluorescence with the help of various indices and criteria to evaluate the measurements show heterogeneity in studies.
Oral hygiene and white spot lesion development are closely linked and patients with poor pre-treatment oral hygiene are more likely to develop WSLs than with fair oral hygiene. 23
Strength and future research recommended
We followed well-established guidelines for the conduction of this analysis that has been undertaken with the thorough searching of the electronic databases. Results of this review are of clinical significance that can be used for choosing the appropriate appliance for the specific orthodontic condition in consideration of post-treatment aesthetic. Clear aligner therapy showed a low incidence of white spot lesions, so it may be a preferred treatment option especially in patients with high caries susceptibility and poor oral hygiene. In addition, clinicians need to encourage their patients regarding oral hygiene maintenance, more during fixed appliance treatment.
Due to lack of high-level evidence regarding this topic, more randomized clinical trials with proper design are required to draw a definite conclusion. Ideally white spot lesion should be studied after debonding because bracket would interfere with adequate assessment of the tooth surface and short-term study will not conclude definite results.
Limitations
There are some limitations to the present review mainly because of the limited number of studies found, in which one study was presented with low quality or high risk of bias. There are limitations to the generalizability of our results due to the presence of severe heterogeneity with respect to sample size, method of WSLs recording, parameters taken, age group, gender variation, and treatment duration. Based on the analysis, conclusive evidence of the outcome is low.
Conclusion
Based on all the studies included in this review, the following conclusion can be made:
Incidence of white spot lesions was less in patients under clear aligner group compared to fixed orthodontic treatment group.
Size of the white spot lesion was larger in subjects with clear aligner therapy than subjects with traditional braces but mineral loss associated with clear aligners were lesser than fixed appliances.
However, more low risk of bias studies with proper methodological qualities are required to be conducted in the near future to strengthen the conclusive evidence.