Introduction
Sometimes there can be anatomical and morphological variations of the teeth which plays a decisive role in treatment planning, so that the objectives of our treatment are fulfilled.1, 2 Among the numerous variations that can occur in morphology of the teeth, one of them is collum angle which may be varied in different situations, especially in maxillary incisors.3 According to some concepts by different authors collum angle is critical for normal development of the permanent dentition and plays an vital role in diagnosis and treatment planning. The necessary amount of palatal root torque which is often required in maxillary incisor region may be influenced by a particular collum angle present, which may sometimes cause the roots of maxillary incisors to come in contact with either labial or lingual cortical plate of the bone during torqueing procedure which may affect the dynamics of mastication especially during loading activity.1 During bonding procedures collum angle can affect the positioning of brackets in vertical dimension and the final root torque that can be expressed.4
Collum angle when measured can vary in different malocclusion groups.1, 4, 5 Collum angle of mandibular central incisor in Class I and Class III malocclusions was assessed by Wang et al. 5 Most of the studies that had been carried out reported that, in Class II division 2 malocclusion cases, collum angle of the maxillary central incisors was increased.1, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15 Collum angle of incisors in Class I, Class II division 1 and division 2 malocclusions was analysed by Feres et al,16 Li et al. compared and evaluated the right and left sides only between Class I and Class II division 2 malocclusion cases. 15 In Class III malocclusion cases prognathic mandible can trap the maxillary incisors and restrain them which may lead to the increase in collum angle. 17 Collum angle is most often assessed routinely from lateral cephalograms, 1, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 17, 18 but there can be different types of landmark identification errors, besides that lateral cephalogram is a 2D image which may be associated with superimposition of adjacent anatomical structures2 and inability to make measurements in all the three dimensions.
During surgical-orthodontic treatment planning of impacted maxillary canines, correct diagnosis requires not only to localize the malposed canines in three dimensions, but also there is need to assess the precise relationship of malposed canines and their impact on the adjacent anatomical structures like bone and adjacent teeth.19, 20, 21 The risk of root resorption can be minimized to a greater extent if we detect any aberrant contact between the impacted canine and roots of permanent teeth especially maxillary incisors.22 The 3D Cone Beam Computed Tomography (CBCT) can be used to accurately assess the collum angle in different situations and overcome these inherent disadvantages of lateral cephalogram. There are little research studies available that have evaluated and compared the collum angle of maxillary central and lateral incisors in subjects with maxillary canine impaction using CBCT. Therefore, the aim of this study was to quantify any variation and compare the collum angle of maxillary central and lateral incisor teeth in subjects with maxillary canine impaction with non impaction side using CBCT.
Materials and Methods
This research study was conducted after getting the ethical approval from the ethical clearance committee government dental college and hospital srinagar, jammu and kashmir. This study was carried out by analysing the CBCT images of thirty patients who visited the department of orthodontics government dental college and hospital srinagar for the treatment of unilateral maxillary canine impaction. After recieving the informed consent, CBCT scans of these patients were used for data collection.
Inclusion criteria
Full set of permanent anterior teeth present with complete radiographic visibility of root formation.
Unilateral permanent maxillary canine impaction.
Unilateral permanent maxillary canine impaction without cleft lip and palate.
Unilateral permanent maxillary canine impaction without any craniofacial syndrome.
Image acquisition
CBCT images were taken with NewTom Giano HR 3D CEPH CBCT machine. The CBCT images were taken with the medium field of view(FOV), height- min 1650 mm (65 in) - max 2410 mm (95 in), scan time-18 seconds, 90KVp, 1-10 mAs (pulsed mode) 0.5mm focal spot, voxel size (micrometer): minimum slice thickness 75 microns. CBCT images were generated in all the axial, sagittal and coronal planes and stored in DICOM format.
Measurement method
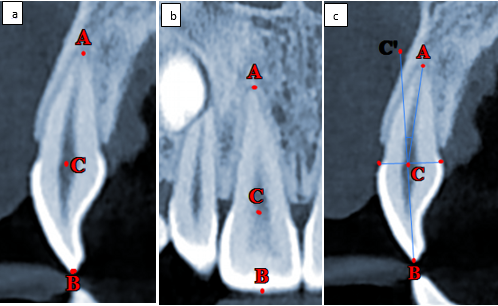
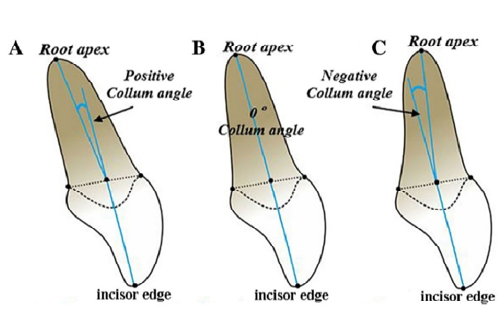
Multiplanar Reformation images of CBCT were selected, in which the sagittal and coronal slices were selected for measurement of collum angle. Sagittal and coronal planes were oriented to Cemento Enamel Junction (CEJ) of the tooth in which the collum angle was to be measured. For the measurement of collum angle in sagittal section, this section was acquired by orienting the sagittal plane to the tooth long axis. The midpoint on the mesiodistal width of the incisal edge in labial view is called incision superius (B). This point was obtained by orienting the coronal plane to the tooth long axis to generate the labial view on which incision superius (B) was constructed. Similarly, the root apex (A) was constructed by orienting the coronal and sagittal section to the apical portion of the root. The midpoint of cementoenamel junction in labiolingual dimension on sagittal section was constructed and was called point (C). The sagittal plane was oriented in such a way that it passed through both incision superius and root apex. Thus, the following landmarks were identified (figure 1a,1b,1c). The long axis of the crown was constructed from the incision superius to point C and extended beyond the CEJ to point C'. The long axis of the root was constructed from point C to root apex. The collum angle (nC'CA) was considered to be positive when the long axis of crown was lingual to the long axis of root (figure 2a). A normal value is assigned when the crown long axis and long axis of root are in same plane (figure 2b). A negative value is assigned when the crown long axis was situated facial to root axis5 (figure 2c). A similar method was applied for the measurement of the collum angle of maxillary central and lateral incisor on both sides of CBCT sample of thirty patients.
Statistical Analysis
The recorded data was compiled and entered in a spreadsheet (Microsoft Excel) and then exported to data editor of SPSS Version 20.0 (SPSS Inc., Chicago, Illinois, USA). Statistical software SPSS (version 20.0) and Microsoft Excel were used to carry out the statistical analysis of data. Descriptive statistical analysis was first done and data were expressed as Mean±SD. Student’s independent t-test was employed was used to assess the mean collum angle of the corresponding maxillary central and lateral incisor of the right and left side. A probability value 0.05 was taken as the cut off for statistical significance.
Results
The collum angle of corresponding right and left side teeth were averaged. Thus, the mean±standard deviation and standard error of the collum angle (n-30) were generated for maxillary central incisor and lateral incisor on both sides. The mean±sd of the maxillary central incisor on impacted and non impacted side was 1.39±7.16 and 2.33±5.86 respectively with a p value of 0.282, while as the mean±sd of the maxillary lateral incisor on impacted and non impacted side was 3.09±6.26 and 5.24±5.28 respectively with a p value of 0.060 which was considered as statistically insignificant between the two sides as shown in the tables I and II below:
Discussion
During the transition from primary dentition to permanent dentition multiple anomalies can occur which may result in the aberrant development of the permanent dentition, among the various developmental disturbances that can occur, eruption disturbances are the most frequently occurring events like impaction of the permanent teeth. After the Permanent maxillary third molars, maxillary canines are the second most frequently impacted teeth with increased prevalence rate in the general population because they have a prolonged development period in maxilla, canines have large root to develop and a long extended tortuous path of eruption compared to other teeth.23 Also, existence of any retained primary teeth or any other pathology like cysts, tumors in the eruption path is an important factor for delaying maxillary canines from eruption.24
Canines form the corner teeth and play a pivotal role in both function and esthetics of the face. Rather than focusing on surgical disimpaction of the impacted canines, there has been a paradigm shift and orthodontists are more concerned about the importance of canine guided occlusion and are utilising different imaging modalities and effective treatment techniques for preserving impacted maxillary canines.3 Therefore, the localization and categorization of impacted canines is necessary for their optimal management. 25 Adjacent anatomic structures also should be analysed while localizing the impacted canines. The roots of adjacent teeth may come in contact with the impacted teeth which may have resorptive effect on both of them.25 According to some concepts by different authors collum angle is important for normal development of the dentition and plays an important role in diagnosis and treatment planning. The necessary amount of palatal root torque which is often required in maxillary incisor region may be influenced by a particular collum angle present, which may sometimes cause the roots of maxillary incisors to come in contact with either labial or lingual cortical plate of the bone during torqueing procedures which may affect the dynamics of mastication especially during loading activity.11 During bonding procedures collum angle can affect the positioning of brackets in vertical dimensions and the final root torque that can be expressed. 4
Apart from influence of hereditary, 26 pressure of lower lip on upper incisors, 27 and excessively high lip Line, 28 which have been considered as the possible etiological factors for the development of collum angle, genesis of crown and root can also differ which could also be a possible etiological factor. While the morphological development of the tooth crown is predominantly under genetic control, but the root form appears to be influenced by local environmental factors. 29 The skeletal and the tooth size characteristic appearance in Class II division 2 malocclusion cases is uniquely influenced by genetic component as suggested by Peck et al. and Fourneron et al. 30, 31 Some pathognomonic features of Class II division 2 malocclusion as described by Prasad et al. were similar to those observed by Peck et al. 32 Some dental anomalies are associated with Class II division 2 malocclusion but it is not common in all types of Class II Division 2 malocclusion as reported by Pereira et al. and Basdra et al. 33, 34 Any alteration in the function during root formation may cause variations in the axis of crown and root because of different sequence of crown and root development. 35 A normal collum angle which is most often seen in the central incisors of Class I and Class II division 1 could be because of physiological pressure from the tongue on the lingual side and lips on the labial side which results in the proper eruptive guidance as reported by Harris et al. 17 For torque expression collum angle is critically important when using a straight wire appliance. 4 The shape of the labial surface of the teeth is also of particular importance when using a straight wire appliance since it was presumed that there was no morphological variations on the facial surface of the anterior teeth and the shape of all anterior teeth is same for all patients. 36 Variations in labial crown morphology and crown root angulation may result in different torque expression when using the same archwire wire in same preadjusted edgewise appliance system as demonstrated by another study. 37 Stress concentration has been reported to be lower in curved tooth during retraction as per Heravi et al. 38 The centre of rotation moves cervically in conditions with increased collum angle and the stress strain distribution increases and the amount of intrusion would decrease and vice versa as reported by Pai et al. 39 The use of similar angles in the third order can vary especially in Class II division 2 malocclusions as studied by Knosel et al. 40 So multiple factors may be responsible for decreased collum angle as mentioned above,
So the main purpose of our study was to find out any changes in collum angle on canine impaction side. Our study suggested that the collum angle was decreased on the impacted side when comparison was made with the non impacted side. The collum angle was more decreased for lateral incisor than central incisor on the impacted side, this decrease in collum angle was not observed in every patient with unilateral maxillary permanent canine impaction, however it was found more decreased in those cases in which canine was palatally impacted, low in position and facing maxillary central and lateral incisors on palatal aspect than canines which were high in position above the roots of incisors, those impacted canines which were facing incisors palatally may exert some pressure on the roots during the developing stage which may be a cause of decreased collum angle, however there is no such strong evidence for this cause and needs further research. Our study suggested that maxillary permanent canine impaction may be a cause of decreased collum angle, but there is no strong evidence to support this fact and further investigations and studies need to be done.
Conclusion
Localization of an impacted tooth like permanent maxillary canine makes it imperative to have an accurate investigation of the adjacent anatomical structures like adjacent teeth. Variations in the morphology of the teeth plays a decisive role in accurate diagnosis and formulation of an appropriate treatment plan and its execution per se, so that all the defined objectives of orthodontic treatment are met. One such variation is the collum angle. Our study suggested a decrease in collum angle on impaction side with a more decreased value for lateral incisor than central incisor when compared with non impaction side, but no statistically significant difference was found when comparison was made between impaction and non-impaction side.