- Visibility 133 Views
- Downloads 10 Downloads
- DOI 10.18231/j.jco.2023.038
-
CrossMark

Temporary anchorage devices-steering the treatment of borderline orthognathic case to an orthodontic approach
- Author Details:
-
 Narayana Iyer Ramana Ramya Shree *
Narayana Iyer Ramana Ramya Shree *
-
Aravind S Raju
-
Vinay P Reddy
-
Chandrashekar B S
-
Mahesh CM
-
Nishan Ansari
Introduction
Orthodontics as a specialty deals with various skeletal and dental malrelations. But, the extent to which the case can be treated with a pure orthodontic approach with the use of fixed appliances was limited. With the advent of temporary anchorage devices, our horizons have broadened and these “WONDER SCREWS” have allowed us to tackle more complicated cases while avoiding surgeries. The skeletal anchorage system has revolutionized the way we address different malocclusions. Temporary anchorage devices have developed into important orthodontic adjuncts for expanding the scope of biomechanical therapy and enhancing clinical outcomes.[1]
The envelope of discrepancy is an essential component of treatment planning, not only for appropriate positioning of the anterior and posterior teeth in the alveolar bone but also for restoring stable occlusion. The development of temporary anchorage devices (TADs) has dramatically altered orthodontic treatment planning, it may not be an exaggeration to state that such devices have resulted in a complete paradigm shift within the field of modern orthodontics.[2]
Increased Anterior vertical dimensions have always posed a challenge which usually required a multi-disciplinary approach such as Orthognathic surgery. The drawbacks of this procedure were increased risk of trauma and cost. Mini screws have been an excellent alternative that can provide true intrusion minimizing the potential side effects.
This case report is focused on showcasing the successful management of the case required to improve the esthetics and function of an adult male through the simultaneous retraction and intrusion of the whole anterior segment ending the case in Class II molar relation.[2] The treatment objectives were achieved through the retraction of the maxillary anteriors using TADs as anchorage and intrusion using the TADs.
Diagnosis and treatment planning
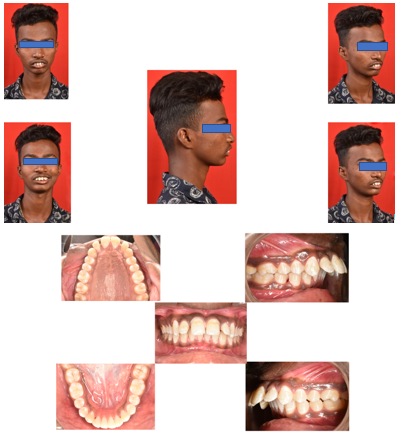
An 18-year-old non-growing male patient came to the department with the chief complaint of forwardly placed upper front teeth region. On clinical examination, the Patient had a convex profile with a posteriorly divergent face and a steep mandibular plane with potentially incompetent lips.
Intraoral examination revealed spacing in the upper anterior teeth with Angle’s class II molar relation and end on canine relation bilaterally with an overjet of 12 mm and overbite of 6 mm (100%) with a shift in lower dental midline towards the patient’s right side as shown in[Figure 1].
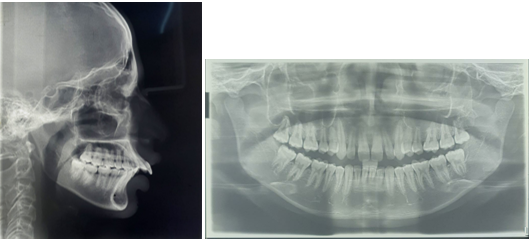
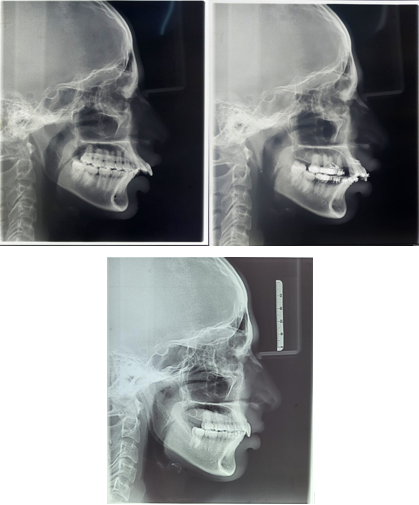
Cephalometric examination revealed that the patient had a class II skeletal base with decreased mandibular length and proclined upper and lower incisors. The patient displayed a vertical growth pattern with a prominent upper lip and a lip strain of 7 mm as shown in [Figure 2].
Treatment Objectives
The treatment objectives included
Correction of skeletal class II relation
Correction of proclined and forwardly placed upper and lower anterior teeth
Correction of upper anterior teeth spacing
Correction of rotations
Correction of overjet and overbite
Correction of potentially incompetent lips
Correction of lip strain
As the patient was past the growing age, it was decided to treat the case by orthodontic camouflage. Extraction of upper first premolars were planned to reduce the overjet and overbite. Temporary anchorage devices were planned for both intrusion and retraction because anchorage conservation was critical. Interproximal stripping was planned in the lower anterior segment because the space requirement was less than 2.5 mm.
Treatment Progress
MBT prescription 0.022” slot (American Orthodontics, Mini master series) brackets were bonded on the upper and lower arches. Leveling and alignment were carried out using NiTi archwires. Keeping in view clinical and cephalometric analysis, the extraction of upper first premolars was performed for the correction of increased overjet and overbite. The versatility of MBT was taken advantage of by bonding the contralateral lower second molar tube on the upper first molar which would help it express the additional mesial tip establishing proper contact between the upper 1st molar and second premolar.
Two titanium mini-screws of dimension 1.4*6 mm (Fav Anchor) was placed between upper lateral incisor and canine to aid in intrusion. After achieving 3 mm of intrusion, two inter radicular implants measuring 1.6*8 mm (Fav Anchor) were placed in between the maxillary 2nd premolar and 1st molar for retraction of the anterior dentition.
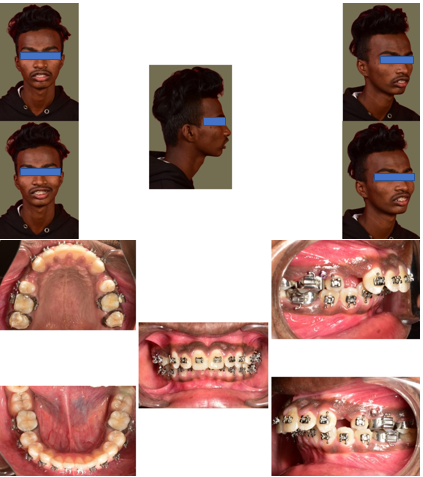
Treatment Records are Displayed in [Figure 3]
Interproximal reduction of 2 mm was done in respect to lower anteriors for levelling and alignment and correction of midline.
Elastic traction using a power chain from the posterior TADs was directed to the hooks crimped onto the anterior segment of 19*25 SS wire just distal to the lateral incisor brackets in order to retract the anterior segment. The force was measured to be 150 grams per side using a Dontrix force gauge. An elastic chain was placed from the archwire to the anterior implants for intrusion. The force for intrusion was measured to be 60 grams.
In eight months, the anterior segment was retracted, and the deep bite was also corrected. The lower arch was stabilized passively with a 19*25 SS wire.
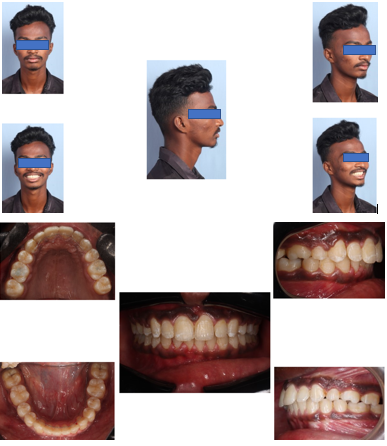
Retraction was completed in 8 months with the proper establishment of contact points as shown in [Figure 4].
Finishing and Retention
Finishing was carried out on a 19*25 TMA and light settling elastics on 0.018 SS were used for settling following which the brackets were debonded. Begg wrap-around retainers were given in both upper and lower arches along with permanent lingual retainers bonded on the upper and lower anterior teeth.
Treatment Outcome
A balanced and pleasing profile with an esthetic and consonant smile was achieved along with harmony between the upper and lower lips, lip competence, and bilateral Class I canine relationships. The occlusion was stabilized in Angle’s class II molar relation as the patient had a good functional occlusion. The dental midlines were coinciding, and no muscle or joint problems developed during the treatment.
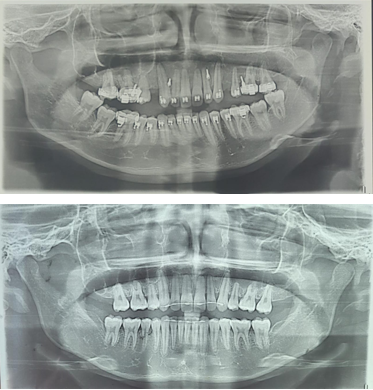
A panoramic radiograph was taken prior to debonding showing acceptable root angulations with little evidence of root or bone resorption as shown in [Figure 5].
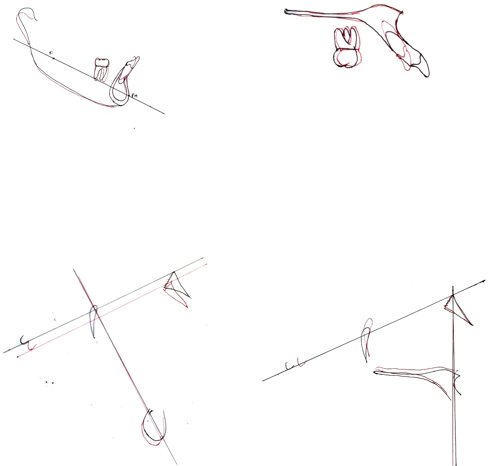
The overjet was corrected, addressing the patient’s initial complaint of proclined teeth and protruding lips as shown in cephalograms and superimpositions ([Figure 6], [Figure 7]).
The cephalometric values showing the treatment outcome are mentioned in [Table 1].
|
Variable |
Norms |
Pre-treatment |
Post treatment |
|
SNA |
82º |
82º |
81º |
|
80º |
78º |
78º |
|
|
ANB |
2º |
4º |
3º |
|
U1-NA |
22º/4 MM |
45º/14 MM |
30º/4 MM |
|
L1-NB |
25º/4 MM |
30º/8 MM |
30º/5 MM |
|
IMPA |
90º |
100º |
100º |
|
Y-AXIS |
66º |
60º |
59.5º |
|
H Line Angle |
8º-15º |
23º |
22º |
|
Naso Labial Angle |
102º |
59º |
78º |
Discussion
The lack of growth potential in adult skeletal class II patients makes it impossible to perform growth modification treatments like functional jaw orthopedics. Despite the fact that the treatment plan is easily established in severe skeletal class II adult patients, it is difficult to reach this decision in borderline cases. Although orthognathic surgery techniques have advanced considerably and are now less traumatic than in the past, it may still be difficult to convince patients and their parents that they should undergo orthognathic surgery. When this is the case, the best way to achieve the desired results is by performing camouflage treatment.[3]
The need for absolute anchorage in our case was because of the Angle’s Class II molar relation of the patient which warranted no further anchor loss which would result in mesialisation of maxillary molars. So, inter radicular implants were a proven choice for the retraction of the maxillary anterior dentition.[4]
Incorporation of miniscrews negated the side effects of anchorage taxation on the posterior segment because the retraction force was not reciprocal.as a result, the entire arch or the anterior segment rotates around the center of resistance.
Class II malocclusions can be treated by several methods keeping in mind various characteristics such as anteroposterior discrepancy, age, and patient compliance. Extraction of only upper first premolars is preferred when there is an increased overjet with minimal to no discrepancy in the mandibular arch.[5] In a study conducted by Janson et al, he concluded that finishing Class II malocclusion treatment with the molars in a Class II relationship has similar occlusal stability as finishing with the molars in a Class I relationship.[6] Because the patient had a stable functional class II occlusion, it was decided to finish the case with Angle’s Class II molar relation and class I canine relation.
The stability of the molar correction from class II to class I is questionable because as we go anterior to the alveolar segment the thickness of the alveolar segment reduces which compromises the stability as the crowns are tipped forward leaving the roots behind.
For the deep bite correction with control over subsequent flaring of the incisors, two mini-implant was placed in between the two central incisors to achieve true intrusion. An overbite correction of 3 mm was achieved. There is sufficient evidence of the usage of two mini-implants over one mini-implant to avoid flaring[7] when placed at the center of resistance of maxillary anterior dentition.
Superimpositions of pre-and post-treatment cephalograms were performed to assess the treatment outcome.
Peer assessment rating was performed objectively to assess the treatment outcome and it was observed that there was an increase in PAR score to 34 and showed 91.8% improvement which according to Richmond Et al.[8] concluded a high standard of treatment.
Conclusion
Using Temporary anchorage devices as an adjunct, we could simultaneously intrude and retract the maxillary anterior and achieve an ideal overjet and overbite.
Source of Funding
None.
Conflict of Interest
None.
References
- T Ono. Should the “envelope of discrepancy” be revised in the era of three-dimensional imaging?. J World Fed Orthod 2020. [Google Scholar]
- A Venugopal, P Manzano, S Rengalakshmi. A novel temporary anchorage device aided sectional mechanics for simultaneous orthodontic retraction and intrusion. Case Reports in Dentistry 2020. [Google Scholar] [Crossref]
- OS Cankaya, F Celebi, AA Bicakci. Effects of different nose types on class II treatments for female patients. Progress in Orthodontics 2019. [Google Scholar]
- PJ Vibhute. Optimizing anterior en masse retraction with miniscrew anchorage. Case Rep Dent 2011. [Google Scholar] [Crossref]
- G Janson, AC Brambilla, JF Henriques, MR De Freitas, LS Neves. Class II treatment success rate in 2- and 4-premolar extraction protocols. Am J Orthod Dentofac Orthop 2004. [Google Scholar]
- G Janson, L T Camardella, J D Araki, M R De Freitas, A Pinzan. Treatment stability in patients with class II malocclusion treated with 2 maxillary premolar extractions or without extractions. Am J Orthod Dentofacial Orthop 2010. [Google Scholar]
- AV Hernández, LG Zubeldia, RL García. One versus two anterior miniscrews for correcting upper incisor overbite and angulation: A retrospective comparative study. Prog Orthod 2020. [Google Scholar] [Crossref]
- S Richmond, WC Shaw, CT Roberts, M Andrews. The PAR index (peer assessment rating): methods to determine outcome of orthodontic treatment in terms of improvement and standards. Eur J Orthod 1992. [Google Scholar]