Introduction
Facial feminization surgery (FFS) is the sequential set of the procedures where the aim must be to feminize the face. Male to female transition for the transsexual patients must be undertaken by these procedures. However, there must be the small group of females who want these types of surgeries for further feminization of their facial masculine aspects. The sequence of the procedures include forehead reduction, lip lift, contouring of orbital rim, scalp advancement, rhinoplasty, cheek implants, brow lift, removal of the buccal fat pads, mandibular angle shave and taper, masseter reduction, genioplasty, and dermis graft to the upper lip and also thyroid shave. FFS was evolved and fashioned by Dr Douglas Ousterhout of San Francisco, California, USA, in between 1980s and 1990s. He inspected a number of dry skulls in the collection of Atkinson skull at the University of San Francisco and further glanced at the various male and female features regarding to the forehead.1 On the basis of his findings he was allowed to evolve different surgical procedures to shape the forehead with the aim to feminize it. The particular procedures among the facial feminization surgery of the specific interest to the orthognathic surgeon include, forehead reduction, orbital rim contouring, cheek implants, rhinoplasty, mandibular angle shave and taper and genioplasty.1
Variation of male and female faces according to aesthetics
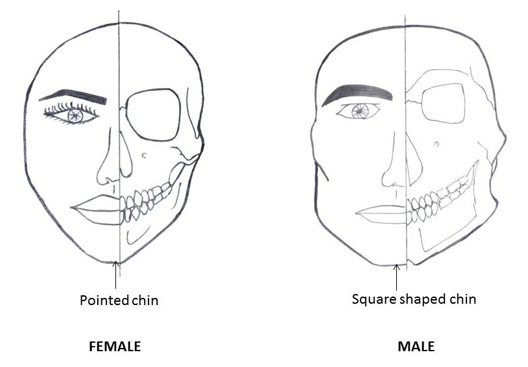
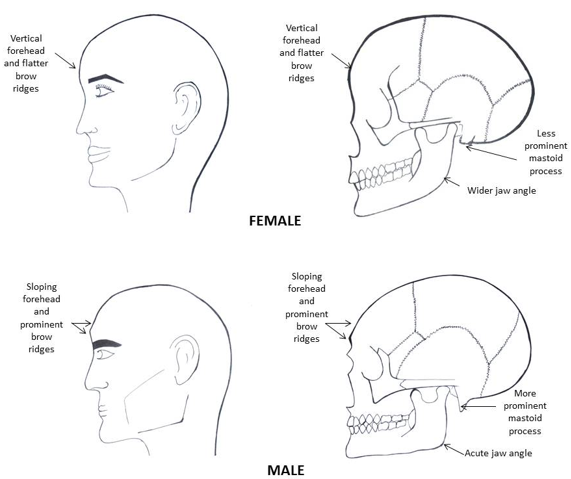
It must be the essential significance for the orthognathic surgeon to have the recognition of the rudimentary variations between the faces of male and female. Feminization of the face is all about the transforming the sharp-angled characteristics to the further rounded one. In the process of feminizing the face should be the chief concern that the facial size that has to be in the proportion with the rest of the body.2 All orthognathic surgeons should be aware about the transverse thirds as well as the vertical fifths of the face as the proportion is the chief characteristic. Examination regarding the female facial features demonstrates the further heart-shaped or else in the triangular manner in which the base of the upturn triangle must be stood for the imaginary line drawn in between the most prominent part of the bone of the cheek and the chin point represents the apex of the triangle. The facial features of the female must be pulpy as well as further rounded or elliptical, with the squashy and curvy form. Male faces are usually square as well as angulated along with the brawny jaw and chin frequently in concurrence with the M-shaped hairline. Longer the chin and lower jaw in the male is by as much as 20%,3 and is frequently more prominent in the overall profile with the bossing forehead which may be because of large frontal sinus and thick supraorbital ridges. In females, the angle at the glabella which is formed by the nose and frontal part of the forehead is usually acute. Female noses are shorter and smaller with tapered bridges and also ala bases, often with upturning of the nasal tip which will give the more obtuse nasolabial angle. Male cheeks should be flat whereas female cheeks can be entirely protuberant as they project more anterior and are higher with some associated cheek hollowing underneath, which provides further accentuation. The male chin is often long, square and angulated while female chins are shorter, narrower and more pointed. The mandible in the male has a prominent angle with lipping of the bone due to the masseter muscle attachment and it is wider than in the female. The oblique ridge is thick and the masseter muscle is often bulkier. (Figure 1, Figure 2)
Surgical procedures in FFS with the special interest of orthognathic surgeon
The characteristic surgical procedures in FFS with the interest of the orthognathic surgeon include the forehead reduction and orbital rim contouring, rhinoplasty, cheek implants, angle shave and taper and genioplasty.4
Forehead Reduction
Forehead shape classification
Group I: Group I includes mild or moderate prominence at the area of eyebrows and bossing abnormality as well as the absence of the bony thickness in front of the frontal sinuses. The reduction must be carried out along with the acrylic burr in order to reach the preferential contour. 4
Group II: Group II cases have the normal brows, mild to moderate projection as well as thick bone present anterior to the frontal sinuses. The reduction of this bone can be achieved in this Group, but it may become fairly thin. As soon as the reduction of the bossing is carried out, there must be the forehead concavity which is present superior to the bossing that requires the filling of bone cement.4
Group III: In group III cases, there is extra fullness of brows and also excessive reduction of the anterior bony table which is anterior to the frontal sinus is required. Osteotomy, reshaping and further fixing with titanium mini-plate osteosynthesis is done for achieving best results in Group III cases. It can be appreciated that the frontal sinus is the asymmetrical structure. To feminize the face, the acute angle at the glabella which is formed by the nose and bossing area converted into the obtuse angle. As authors’ perspective, majority of the bone reduction procedures are undertaken in Group III only.4
Planning and surgical procedure
The coronal, sagittal and axial planes and anterior bony table are estimated by the CBCT, which is 2 to 3 mm in the thickness in most of the cases, away from the midline septum. Axial and sagittal sections are the most important parameters for the Group III surgical cases. The vertical length of the anterior table from the superior-most aspect to the glabella is measured as is the horizontal maximum dimension. These quantifications are set down as these will be the premise regarding the markings which will be made at the time of the operation. Bone reduction procedure is achieved by acrylic trimming burr with fast motor and in addition contouring of frontal process of zygomas are also carried out, if required in Group I and II cases. Ousterhout basically introduced the benefits of methylmethacrylate onlay implants in Group II cases, though the use of bone cement has now superseded this. Osteotomy is required for the Group III cases.5
Rhinoplasty
The aim and objectives for the feminizing rhinoplasty, is to lessen the piece of the dorsal protuberance and to taper the bridge of the nose by fracturing the nasal bones. In the feminization procedure, the dorsum should be straight but some individual want the curvature in dorsum, so it should be accordingly. Skin excision must be carried out at the nasal sills for the reduction of the nostril aperture. Nose should be in the proportion of the rest of the face as small nose will appear abnormal on the large face. Usually, rhinoplasty is performed with the combination of forehead reduction. If an open procedure is used in the combination with the lip lift, then the columella skin flap must be lifted up from the nasal sill to include the lip lift skin excision instead of mid-columella area which is normal. 6
Cheek Augmentation
Cheek implants are one of the principal surgical procedures among the facial feminization surgery. An inverted triangle in which chin is the apex and an imaginary line between the prominences of the cheeks is the base must be the most feminine profile and it will provide the most aesthetic appearance of the lower two- thirds of the face. This can successfully be performed by the cheek augmentation with the implants.6
Planning and Surgical Procedure
After infiltration of the local anaesthetic an adequate pocket will be anatomized before the placement and this must incorporate dissection along with the zygomatic arches to confirm that the implants place passively above the rudimentary bone as they are fluffy in the proper location. To achieve the symmetrical implants must be challenging. Once the orthognathic surgeon is assured about the aesthetic look, he can fit the implants. Prior to the insertion of implants, they are immersed in the suitable antibiotic solution, after that screwed into the elementary bone along with the two 2.0 mm titanium screws which has least 6.0 mm of length on each side to prevent further migration as well as rotation. Some degree of malar fat pad lifting is also provided by the cheek implants.5
3/0 Vicryl Rapide suture (Ethicon Inc.) is used for the closing of oral mucosa.
Angle shave and taper
A sharp-angled mandible is the strong masculine characteristic; therefore the mandible contouring must be needed in many cases of feminization surgery. An angulated mandible is usually too square and also associated with the bulk of the masseter that will lead to the extra width of the mandible. This mandible contouring is called as Angle shave and taper. 7
Planning and surgical procedure
For the estimation of mandibular angle and chin, an orthopantomogram (OPG) is the essential radiograph. Followed by local anaesthesia, the entire procedure will be performed through the mouth with an incision from high on the external oblique ridge to the area of first molar. Best retraction is required. Reduction of the cortical bone is achieved by exposing the cancellous bone along with the high speed acrylic burr for the reduction of the prominence of mandibular angle as well as the external oblique ridge up to the mental foramen. The inferior dental nerve, inferior dental canal and tooth roots must be prevented from the exposure during the procedure. 5
Genioplasty
The aims and objectives of the feminizing genioplasty are to taper the high angled chin which is masculine. Usually, the basic essentiality is the reduction of the excessive vertical chin height.3 Chin osteotomies provide much superior results rather than the contouring alone, though some of the additional contouring is also achieved.
Planning and surgical procedure
Presence of the tooth roots and also any associated pathology can be assessed by the orthopantomogram (OPG). Tapering the chin is directly performed by the removal of a pre-established hunk of midline bone, which will be osteotomized and removed. The two remaining halves of the chin are brought together in the midline and stabilize with the 1.3 mm X-shaped titanium mini-plate and two further 3-hole mini-plates placed laterally to secure the fragments. 3/0 Vicryl Rapide suture (Ethicon Inc.) is used for the mentalis muscle as well as oral mucosa closure.5
Lip lift
The aims and objectives of the lip lift procedure are to shorten the upper lip, which will provide the more feminine look because of having shorter upper lip. Smaller upper lip will provide more exposure of the maxillary incisors both at rest position as well as on smiling. Upper lip augmentation with dermal grafts or fillers changes the shape and also increases the prominence of an upper lip for the feminine appearance. The upper lip incision lifts as well as the augmentation is generally well hidden in between the base of the nose and the upper lip. The upper lip lift includes excision of the bullhorn-shaped piece of skin which is from under the nose. The skin is raised and then sutured to lift the upper lip.6
Discussion
There is very restricted role of the orthognathic surgeon in the procedures of facial feminization, because this facial surgical area is much more specialized and ideally involved surgeons can be the part of a multidisciplinary team of doctors. FFS includes a bulk of craniomaxillofacial surgical procedures whose only objective is the transformation of the masculine face into the feminine one. There must be no attempt for embellish or renovate, though these outcomes must be the by-product of these feminization techniques. The chief aim and objective must be to pass the transgender and male who wants to live as a female independently in day to day community and to combine into the society. The quality care for transgender individual is skill-fully described, though too lessen is written in the World Professional Association for Transgender Health (WPATH) literature with particularly in regard to FFS procedures. 8 Ousterhout was the pioneer of the facial feminization surgery. He performed anthropological studies on the few hundred dried skulls at the Atkinson skull collection at the University of San Francisco and identified particular characteristics and features that can be different for female and male human skulls. 1 His findings allowed the evolution of the surgical procedures on the particular areas of face and skull those were acquiescent to feminization. Most of the transgender females have generally lived the quality life after undergoing FFS, which is usually the initial surgery they had. This is very important for those who want to unite with women in day to day life. Most of the patients are extraordinarily well informed for the FFS. Some in addition have had photographs prepared from a virtual FFS website indicating what they are likely to look like following various aspects of this surgery. All patients are photographed and detailed informed consent is taken. Most of the transgender patients take numerous hormones which includes estrogens such as estradiol, anti-androgens such as cyproterone and gonadorelin analogues. Spironolactone is generally advised because of its properties of testosterone suppressant. Hormone medication should not be stopped for the patients undergoing with FFS, but prophylaxis and full venous thromboembolism assessment must be given for the procedure. There are no larger studies for this aspect of care in the clinical surgical terms, but the experience of authors proposes the satisfaction of the patients is generally high followed by these procedures. Mental health issues are always with the trans women and it will diminish the quality of life. FFS coupled with gender reassignment surgical procedure has been appeared to be correlated with the best quality of life and mental health.9
Conclusion
There is a broad range of FFS surgical procedures with the aim to transform the masculine facial characteristic to the feminine one. On the conclusion, facial feminization procedures have been found to be extremely successful procedures for both men who wish to convert in women and also for women who want more feminine facial features. Because of wide range of FFS procedures accessible, it is the chief concern to acknowledge that all the patients will not be in need of all the procedures as well as all the patients must be assessed and also treatment planned by the team of multidisciplinary departments to guarantee that the best outcomes will be carried out.