Introduction
The maxillary sinus is a para-nasal sinus, which is a bilateral air-filled cavity pneumatising the maxilla.1 It is the first para-nasal sinus to form with a volume of 6-8 cubic cm at birth.2 The alveolar process of the maxilla forms the floor of the maxillary sinus with premolar and molar roots in close proximity to the sinus floor.3 This relation makes the floor of the maxillary sinus inferior to the nasal floor by 4-5 mm.4 The maxillary sinus along with other paranasal sinuses is involved in various physiological functions like moisturizing the inspired air, equilibrating atmospheric pressure changes, adding resonance to voice, increasing the area of olfactory mucosa, reducing the weight of the cranium.5
The close anatomic relation of the maxillary sinus with the maxillary dentoalveolar complex makes it imperative to evaluate the sinus preoperative to various dental interventions such as endodontic surgery of maxillary posterior teeth,6 prosthetic rehabilitation using dental implant or surgical extraction of impacted maxillary posterior teeth.7 Impacted maxillary teeth, especially canine being closely related to the sinus might affect its shape and volume.3 Also, the invasion of sinus wall in between the maxillary teeth roots may influence the orthodontic tooth movement.4, 8 Anchorage devices in the form of mini-implants are placed in close proximity to maxillary teeth roots and sinus, therefore evaluation of sinus is necessary during treatment planning to prevent iatrogenic injury.9
The dimensions and volume of the maxillary sinus correlated among different age groups, genders, malocclusion types, patients with and without posterior crossbite and patients with unilateral cleft lip and palate have been reported. However, there have been limited studies (mostly 2D) evaluating the dimensions and volume of the maxillary sinus in various skeletal facial types. Hence, the present 3D study was carried out to evaluate the dimensions and volume of the maxillary sinus along with its distribution among different sagittal and vertical skeletal facial types.
Figure 1
Marking of ROI in axial sections of CBCT image and volume computation using HorosTM software

Figure 2
Assessment of maxillary sinus dimensions in axial and coronal section of CBCT image using NNT image analysis software
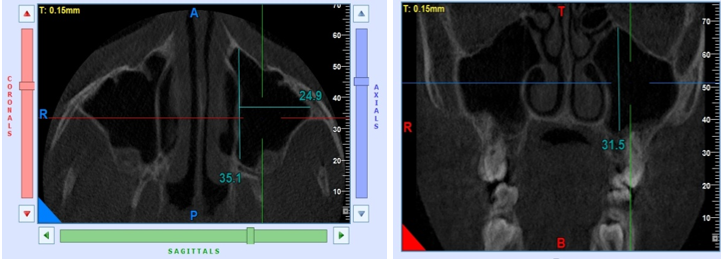
Figure 3
Distribution of means of maxillary sinus volume according to type of divergence and class of malocclusion.

Figure 4
Distribution of means of maxillary sinus dimensions according to type of divergence and class of malocclusion

Table 1
Distribution of mean of maxillary sinus volume and dimensions among differentsagittal and vertical skeletal patterns.
Table 2
Inter-group statistical comparisons of mean maxillary sinus volume and dimensions among different sagittal and vertical skeletal patterns.
Table 3
Inter-group statistical comparisons of mean maxillary sinus volume and dimensions among different sagittal and vertical skeletal patterns.
Materials and Methods
This record-based observational cross-sectional descriptive study was conducted following ethical clearance obtained by the Institutional Ethical Committee (IEC/Oct/2019). Inclusion criteria were (a) Age 18 – 30 years with both genders included (b) availability of good quality, digital copy of pre-treatment lateral cephalogram and CBCT images (c) CBCT images with FOV that encompass complete maxillary sinus (d) availability of a complete set of pre-treatment records including medical case history. Exclusion criteria comprised of (a) Poor quality (low resolution, poor contrast, noisy radiographic images)/incomplete records (b) Syndromic patients including cleft lip and palate patients (c) Medical history suggestive of any systemic disease/condition affecting bone metabolism and sinus morphology (d) History of trauma to jaw bone/prior surgery/ maxillary orthognathic surgery/ ridge augmentation procedures like sinus lift procedure (e) Patients with missing/extracted maxillary posterior teeth (including third molars) (f) Patients with facial asymmetry.
The study sample was selected from pre-treatment records retrieved from the archives of the institution. All records available were obtained by a single operator, qualified and trained radiographer with standard protocol as recommended by the manufacturer from CBCT machine, M/s Cefla Dental Group Italy, Model - NEW TOM GIANO: G-XR-46893and Dental radiography unit (PlanmecaProline XC unit, Finland). The digital copies of the lateral cephalograms were retrieved in DICOM 3.0 format using NNT (NewTom image viewer) analysis software and were transferred to NemocephTM software (Nemotec, version 6.0) for specific automated cephalometric analysis.
The records were then segregated into three sagittal groupsbased on ANB angle as follows:
Each sagittal group was further subdivided into three vertical subgroups based on SN-GoGn angle as follow:
Subgroup A (High angle): (SN-GoGn angle > 380)
Subgroup B (Average angle): (SN-GoGn angle 260-380)
Subgroup C (Low angle): (SN-GoGn angle < 260)
Accordingly, three sagittal groups and nine vertical subgroups were obtained. The CBCT data was transferred to the HorosTM software [GNU Lesser general public license, Version 3 (LGPL-3.0), Horos Project, Annapolis, MD, USA] for volumetric assessment. To assess the volume of the maxillary sinus, every fifth axial section in the serieswas selected from the multi-plane reformation (MPR) view of CBCT(thickness of 150.00μm). The boundary of the maxillary sinus was marked using the ROI (Region of Interest) function of HorosTM software and volume of the maxillary sinus was computed using the “Generate missing ROI” and “Compute ROI volume” functions in the HorosTM software [Figure 1].
The linear dimensional measurements of the maxillary sinus were performed on axial and coronal CBCT images using the “linear scale tool” in NNT analysis software (NewTom image viewer, M/s Cefla Dental Group Italy). The CBCT image with the greatest dimensions in length, width and height of the maxillary sinus was selected [Figure 2]. The length of the maxillary sinus was defined as the longest distance from the most anterior point to the most posterior point of the sinus wall in the axial view. The width is the longest distance perpendicular from the medial wall of the sinus to the most lateral wall of the maxillary sinus in the axial view and height is the longest distance from the lowest point of the sinus floor to the highest point of the sinus roof in the coronal view.
Sample size calculation
The sample size was calculated to describe the confidence interval for mean, considering a population size (number of available records) of 150, for 95% level of confidence and a margin of error of 0.5. Accordingly, a sample size of 69 was calculated. However, to cater for the homogenous subject in each group a sample size of 90 was selected.
Statistical analysis
The data was statistically analyzed using Statistical Package for Social Sciences (SPSS ver 22.0, IBM Corporation, USA) for Microsoft Windows. The inter-group statistical comparison of means of continuous variables was done using Analysis of Variance (ANOVA) with Bonferroni’s multiple group comparisons. To ascertain intra and inter-operator bias three records from each subgroup i.e.,a total of 27 records were randomly selected and retraced after two weeksby the same and another trained operator. The intra-observer and inter-observer correlation coefficient was 0.85 and 0.80 respectively.
Results
The mean maxillary sinus volume among the population was 13.08 (+/- 5.38) cu mm. The distribution of mean sinus volume did not differ significantly across different sagittal and vertical skeletal patterns (P-value>0.05 for all) [Table 1, Table 2, Table 3 ] [Figure 3]. The only statistically significant finding was greater maxillary sinus length in all three types of vertical skeletal patterns of Class I compared to Class III malocclusion (P-value<0.05) [Figure 4].
Discussion
The maxillary sinus is a three-dimensional structure, its evaluation and comparison among different sagittal and vertical skeletal patterns requires three-dimensional imaging. The initial studies used lateral cephalogram and OPG to evaluate and compare the size of the maxillary sinus among different malocclusions, harbouring an inherent error of extra-plotting the size on a two-dimensional image of a three-dimensional structure. Therefore, in the present study, CBCT images were utilized for the measurement of maxillary sinus dimensions and volume computation.
The distribution of the study sample in different sagittal and vertical skeletal patterns was performed on the basis of ANB and SN-GoGn angle as per the method described by Endo T et al.9 and Oksayan R et al. 10. The study by Emirzeoglu M et al. 11was one of the initial studies that utilized a series of CT sectional images to quantify volume of paranasal sinuses. In the present study, volume computation of the maxillary sinus was performed as per the method described by Oksayan R et al. 10
In this study, the results concluded that the distribution of mean sinus volume and dimension do not differ significantly across different sagittal and vertical skeletal patterns. The only statistically significant finding was the greater maxillary sinus length in all three types of vertical skeletal patterns of Class I compared to Class III malocclusion. The present study's finding is consistent with Oksayan R et al. 10 regarding vertical growth patterns. However, Endo T9 et al. revealed that the maxillary sinus length showed a significant positive correlation among upper anterior face height in individuals aged 12-16 years with the aid of cephalometric radiographs.3 Such a correlation could not be established in the present study. Asantogrol F et al.12 described the distribution of maxillary sinus volume among three sagittal skeletal groups based on ANB angle and reported no statistically significant difference between different sagittal skeletal groups.
Orthodontic implications
Orthodontic tooth movement through sinus wall
Orthodontic tooth movement occurs through a coordinated bone modelling and remodelling reaction in both trabecular and cortical bone. However, because of decreased vascularity, the remodelling process in the cortical bone is slow as compared to the trabecular bone. Therefore, cortical bone acts as an anatomic limitation during orthodontic tooth movement. With the increased demand for adult orthodontics, orthodontists are often faced with the challenge of correcting occlusal problems within constrained anatomic limits, such as atrophic alveolar process, and pneumatisation of alveolar process by maxillary sinus. Cortical bone attributed to these anatomic limitations, as such conditions require orthodontic tooth movement through the cortical bone.4 Moving teeth through the maxillary sinus is considered a challenging task in orthodontics, since it requires compensatory new bone apposition, along the sinus wall before bone resorptioncan occur in the direction of tooth movement to maintain the integrity of sinus wall. Along with this, a few additional complications such as root resorption, loss of tooth vitality and perforation of sinus membrane further add to the complexity of the process.13 A systematic review by Sun et al. 8 concluded that presently no evidence-based protocol could be recommended to guide orthodontic tooth movement through the maxillary sinus, however, application of light continuous force appears to be practical and safe.
TAD and sinus extension in posterior maxillary dentoalveolar region
Orthodontic implants/TADs are utilized to reinforce anchorage and ensure predictable dental movements, eliminating the reciprocal effects of conventional mechanics on dental anchor units. 14 The maxillary posterior dentoalveolar region is frequently used as an insertion site for orthodontic implants. The descent of the maxillary sinus floor in theposterior dentoalveolar region makes this area susceptible to complications such as sinus perforation which may culminate in implant failure and/or maxillary sinusitis. 15 As maxillary sinus frequently pneumatise maxillary posterior dentoalveolar process, Liou et al. 16 recommended insertion of mini-screws in infrazygomaticregion at the level of the maxillary first molar, 14-16 mm above, and with an angle of 55 to 70 degree to the maxillary occlusal plane.
A study on adult human dried skulls concluded that sinus perforation is more likely with a 6 mm or greater length mini-screw placed in the infrazygomatic crest and recommended a 6 mm or shorter length screw. 17 However, this site is associated with the emergence of mini-screw head through the alveolar mucosa leading to soft tissue embedment, irritation and infection, therefore, inter-radicular placement of the mini-screw is frequently preferred. 15 Laursen et al. 18 reported that there is an increased risk of sinus perforation with apically inclined insertion in the inter-radicular region and recommended a perpendicular insertion at mid-root level. Studies have reported that even if perforation occurs, interruption of orthodontic treatment or removal of mini-screw is not required. Also, small, uncomplicated perforations healed spontaneously with rare incidence of sinusitis and reduced screw stability.19, 20
Malocclusion and maxillary sinus
As the maxillary sinus forms an integral part of the naso-maxillary complex, many studies relate sinus size with maxillary growth and malocclusion. Two-dimensional evaluation of maxillary sinus area in different malocclusion has been conducted on OPG and lateral cephalogram. 9, 21 The study conducted on OPG of 189 subjects with ages ranging from 6 to 30 years by Oktay H, 21 concluded that there is no difference in maxillary sinus size among different gender, however, in regards to malocclusion, the study reported increased maxillary sinus size in female subjects with Angle Class II malocclusion.Similarly, Endo et al, 9 reported no significant difference in maxillary sinus size among gender and malocclusion. However, an associated finding in the study suggested that subjects with large cranial bases and naso-maxillary complex tend to have large maxillary sinus. Demirtas et al. 22 compared sinus volume in unilateral cleft lip and palate patients and non-cleft controls, reporting smaller sinus volume in the former group while Barbosa et al. 23 reported relatively smaller maxillary sinus volume in unilateral cleft lip and palate patients as compared to bilateral cleft patients.
Conclusion
The following conclusions were drawn from this study:
The mean maxillary sinus volume among the population is 13.08 (+/- 5.38) cu mm.
Distribution of mean sinus volume did not differ significantly across different sagittal and vertical skeletal patterns.
The distribution of maxillary sinus dimensions did not differ significantly across the different skeletal patterns (P-value>0.05). The only statistically significant finding was the greater maxillary sinus length in all three types of vertical skeletal patterns of Class I compared to Class III malocclusion.
Authors’ Contributions
KN- data collection, interpretation of data and writing of protocol and manuscript. SD designed the concept, supervised the workflow and reviewed the paper. SSC participated in concept design and reviewed the paper. DJ assisted in data retrieval from the archieve and preparing the manuscript. All the authors read and approved the final manuscript.