- Visibility 30 Views
- Downloads 9 Downloads
- DOI 10.18231/j.jco.2023.052
-
CrossMark

Correlation of dental arch width and alveolar arch width with facial divergence
- Author Details:
-
 Bharti Goyal *
Bharti Goyal *
-
Sudhir Munjal
-
Ankit Sikri
-
Abhishek Sharma
-
Jasmeet Ryait
-
Rishu Gautam
Introduction
Arch dimensions and arch forms are 2 prime factors in case assessment, diagnosis and treatment planning. The association of malocclusion and facial form has been a focus of orthodontist since early 20th century. Facial growth and development are of deep concern for an orthodontists because the amount and direction of growth will significantly alter the need for orthodontic treatment. [1] In the vertical plane, 3 basic types of facial morphology exist: short, average and long. Person with long face have excessive vertical facial growth which is usually associated with an anterior open bite, increased SN-MPangle, increased Gonial angle and increased maxillo-mandibular plane angle. The short face types have reduced vertical growth associated with deep overbite, reduced facial heights, reduced SN-MP angle and reduced FMA.[2] Average face lies between these two types.
In the present day orthodontic practice, newer techniques and materials have introduced for orthodontists convenience and patient comfort with greater precision; preformed archwires have gained popularity. The shape of preformed archwires especially superelastic nitinol wires can’t be altered easily. Hence, the choice of the arch form has become essential when using these superelastic wires. [3] Instability in arch wire changes can result in periodontal breakdown and relapse particularly when intercanine width and intermolar width has been expanded. [4] Therefore, the present study aimed to correlate different Vertical facial types with Dental arch width and Alveolar arch width for the patients in North Indian subpopulation.
Aim and Objectives
To correlate Dental arch width and Alveolar arch width with Facial divergence.
Materials and Methods
The present study was performed on 150 untreated adults reporting to the Department of Orthodontics and Dentofacial Orthopedics, Dasmesh Institute of Research and Dental Sciences, Faridkot Punjab, India. Following inclusion and exclusion criteria were followed.
Inclusion criteria
Patients with full complement of permanent dentition with or without third molars.
Age: 18-25 years.
Exclusion criteria
Patients with previous orthodontic treatment.
Patients having history of trauma.
Patients with craniofacial anomalies, syndromes, cleft lip and palate.
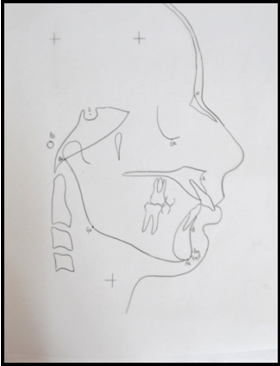
Lateral cephalograms obtained were manually traced by using acetate matte tracing sheet (0.003" thick, 8 x 10") and a 3H drawing pencil. Landmarks (Figure 1) were marked. Cephalometric measurements were obtained. Subjects were divided into 3 groups: Group I (Normodivergent), Group II (Hypodivergent) and Group III (Hyperdivergent) on the basis of cephalometric analysis (SN-MP angle, FMA, Gonial angle & Jarabak’s ratio). The subjects that fall into a particular group according to atleast three parameters out of four were selected
Study model measurements
Measurements were done on maxillary and mandibular casts by using digital caliper (Figure 2). Following measurements were obtained (Table 1).

|
S. No. |
Variable |
Abbreviation |
Definition |
|
(i) Dental Arch Width |
|||
|
1 |
Maxillary Intercanine Width |
(UC-C) |
The distance between the cusp tips of the right and left canines or the center of the wear facets in cases of attrition. |
|
2 |
Maxillary Interpremolar Width |
(UP-P) |
The distance between the cusp tips of the right and left first premolars. |
|
3 |
Maxillary Intermolar Width |
(UM-M) |
The distance between the mesiobuccal cusp tips of the right and left first molars. |
|
4 |
Mandibular Intercanine Width |
(LC-C) |
The distance between the cusp tips of the right and left mandibular canines. |
|
5 |
Mandibular Interpremolar Width |
(LP-P) |
The distance between the cusp tips of the right and left mandibular first premolars. |
|
6 |
Mandibular Intermolar Width |
(LM-M) |
The distance between the most gingival extension of the buccal groove on the first molars or, when the grooves had no distinct terminus on the buccal surface, between points on the groove located at the middle of the buccal surfaces. |
|
(ii) Alveolar Arch Width |
|||
|
1 |
Maxillary Canine Alveolar Width |
(UAC-C) |
The distance between two most prominent points viewed occlusally in canine alveolar region above the cusp tips of the maxillary right and left canines. |
|
2 |
Maxillary Premolar Alveolar Width |
(UAP-P) |
The distance between two most prominent points viewed occlusally in premolar alveolar region above the interdental contact point of the maxillary first and second premolars. |
|
3 |
Maxillary Molar Alveolar Width |
(UAM-M) |
The distance between two most prominent points viewed occlusally in molar alveolar region above the mesiobuccal cusp tips of the maxillary first molars. |
|
4 |
Mandibular Canine Alveolar Width |
(LAC-C) |
The distance between two most prominent points viewed occlusally in canine alveolar region above the cusp tips of the mandibular right and left canines. |
|
5 |
Mandibular Premolar Alveolar Width |
(LAP-P) |
The distance between two most prominent points viewed occlusally in premolar alveolar region above the interdental contact point of the mandibular first and second premolars. |
|
6 |
Mandibular Molar Alveolar Width |
(LAM-M) |
The distance between two most prominent points viewed occlusally in molar alveolar region above the buccal groove of the mandibular first molars. |
Results
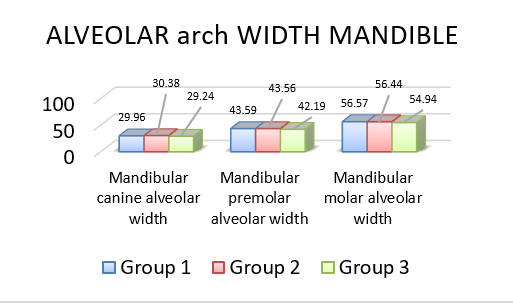
All the data obtained was summarized and analyzed using SPSS software to arrive at specific conclusions. Mean and standard deviation values were calculated for all parameters in each group. Three groups [Group I (Normodivergent), Group II (Hypodivergent) and Group III (Hyperdivergent)] were compared for Dental arch width, Alveolar arch width and Arch length by using one way analysis of variance (ANOVA) as shown in Table 2. ANOVA statistics show significant (p<0.05) correlation for parameters of Dental arch width (Maxillary intercanine width, Maxillary interpremolar width, Maxillary intermolar width, Mandibular intercanine width, Mandibular interpremolar width and Mandibular intermolar width) as shown in Graph 1, 2 and Alveolar arch width (Maxillary canine alveolar width, Maxillary premolar alveolar width, Maxillary molar alveolar width, Mandibular canine alveolar width, Mandibular premolar alveolar width, Mandibular molar alveolar width) as shown in Graph 3, 4. Hyperdivergents had narrower dental and alveolar arch width than hypodivergents.
|
Parameter |
Group 1 (N=52) |
Group 2 (N=54) |
Group 3 (N=44) |
ANOVA |
|
|
(Mean ± S.D.) |
(Mean ± S.D.) |
(Mean ± S.D.) |
F-Value |
P-Value |
|
|
Maxillary Intercanine Width UC-C |
34.98 ± 2.81 |
36.28 ± 3.75 |
33.26 ± 2.94 |
10.725 |
<0.001* |
|
Maxillary Interpremolar Width UP-P |
42.15 ± 2.97 |
43.93 ± 3.26 |
39.92 ± 3.12 |
20.030 |
<0.001* |
|
Maxillary Intermolar Width UM-M |
52.34 ± 3.36 |
53.42 ± 3.34 |
50.50 ± 2.59 |
10.492 |
<0.001* |
|
Mandibular Intercanine Width LC-C |
26.52 ± 2.16 |
27.39 ± 2.52 |
25.78 ± 2.13 |
6.094 |
<0.003* |
|
Mandibular Interpremolar Width LP-P |
34.81 ± 4.47 |
35.86 ± 3.04 |
33.84 ± 2.41 |
4.170 |
<0.017* |
|
Mandibular Intermolar Width LM-M |
50.30 ± 2.87 |
50.63 ± 2.43 |
49.09 ± 2.68 |
4.357 |
<0.015* |
|
Maxillary Canine Alveolar Width UAC-C |
38.20 ± 2.43 |
39.81 ± 3.29 |
36.49 ± 2.45 |
17.318 |
<0.001* |
|
Maxillary Premolar Alveolar Width UAP-P |
49.20 ± 3.14 |
51.05 ± 3.51 |
47.41 ± 2.94 |
15.605 |
<0.001* |
|
Maxillary Molar Alveolar Width UAM-M |
59.00 ± 3.50 |
60.47 ± 3.38 |
57.20 ± 2.77 |
12.222 |
<0.001* |
|
Mandibular Canine Alveolar Width LAC-C |
29.96 ± 2.08 |
30.38 ± 2.47 |
29.24 ± 1.87 |
3.355 |
<0.038* |
|
Mandibular Premolar Alveolar Width LAP-P |
43.59 ± 1.78 |
43.56 ± 3.16 |
42.19 ± 2.35 |
4.713 |
<0.010* |
|
Mandibular Molar Alveolar Width LAM-M |
56.57 ± 2.45 |
56.44 ± 2.74 |
54.94 ± 2.56 |
5.725 |
<0.004* |
Post Hoc Turkey HSD test shows that Dental arch width and Alveolar arch width decreases significantly (p<0.05) from hypodivergents to hyperdivergent (Table 3).
|
Parameter |
Group 1 vs Group 2 |
Group 1 vs Group 3 |
Group 2 vs Group 3 |
|||
|
Mean diff |
P-value |
Mean diff |
P-value |
Mean diff |
P-value |
|
|
Maxillary Intercanine Width UC-C |
-1.30 |
0.096 |
1.72 |
<0.027* |
3.02 |
<0.001* |
|
Maxillary Interpremolar Width UP-P |
-1.78 |
<0.011* |
2.23 |
<0.002* |
4.01 |
<0.001* |
|
Maxillary Intermolar Width UM-M |
-1.08 |
0.185 |
1.84 |
<0.014* |
2.91 |
<0.001* |
|
Mandibular Intercanine Width LC-C |
-0.87 |
0.127 |
0.74 |
0.255 |
1.61 |
<0.002* |
|
Mandibular Interpremolar Width LP-P |
-1.05 |
0.262 |
0.97 |
0.363 |
2.02 |
<0.013* |
|
Mandibular Intermolar Width LM-M |
-0.32 |
0.808 |
1.21 |
0.070 |
1.53 |
<0.014* |
|
Maxillary Canine Alveolar Width UAC-C |
-1.61 |
<0.009* |
1.71 |
<0.009* |
3.31 |
<0.001* |
|
Maxillary Premolar Alveolar Width UAP-P |
-1.86 |
<0.010* |
1.79 |
<0.020* |
3.65 |
<0.001* |
|
Maxillary Molar Alveolar Width UAM-M |
-1.47 |
0.057 |
1.80 |
<0.021* |
3.27 |
<0.001* |
|
Mandibular Canine Alveolar Width LAC-C |
-0.42 |
0.586 |
0.72 |
0.240 |
1.14 |
<0.029* |
|
Mandibular Premolar Alveolar Width LAP-P |
0.03 |
0.998 |
1.40 |
<0.020* |
1.37 |
<0.022* |
|
Mandibular Molar Alveolar Width LAM-M |
0.13 |
0.963 |
1.63 |
<0.007* |
1.50 |
<0.014* |
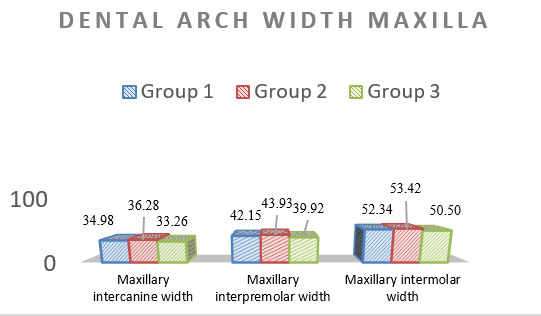
Significant decrease in Maxillary inercanine width, Interpremolar width and Intermolar width from hypodivergents to hyperdivergents.
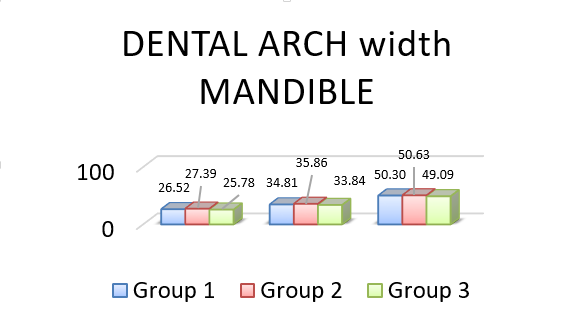
Significant decrease in Mandibular intercanine width, Interpremolar width and Intermolar width from hypodivergents to hyperdivergents.
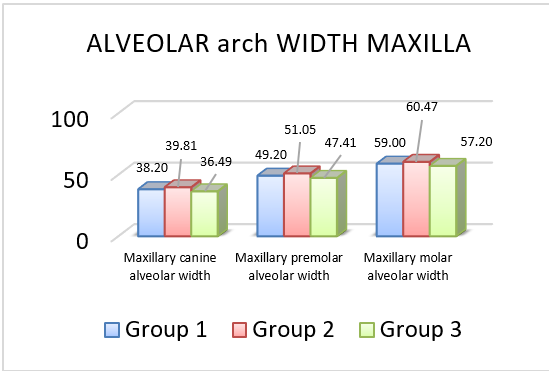
Significant decrease in Maxillary canine alveolar width, Premolar alveolar width and Molar alveolar width from hypodivergents to hyperdivergents.
Discussion
Larger variations found in vertical dimension will affect the clinician’s approach to successful diagnosis, treatment planning and biomechanics. Intergroup comparisons were done between normodivergent, hypodivergent and hyperdivergent subjects for dental arch width, alveolar arch width, arch length and sagittal facial types by using one way analysis of variance (ANOVA) followed by Post Hoc Turkey HSD test. The results drawn from present study showed that there was a statistically significant (p<0.05) inverse relationship between vertical facial morphology and dental arch width at canine, first premolar and first molar region in both maxillary and mandibular arches. These findings were supported by Nasby et al (1972), [5] Khera et al (2012), [6] Prasad et al. (2013), [7] Grippaudo et al. (2013), [8] Jumani, Erum & Ahmed (2014), [9] Alghamadi & Tashkandi (2022) [10] and Yamamoto, Tanikawa & Yamashiro (2023). [11] Statistically significant (p<0.05) inverse relationship found between vertical facial morphology and alveolar arch width at canine, first premolar and first molar region in both maxillary and mandibular arches. These findings were supported by Christie (1977), [12] who found that short-faced men had greater maxillary and mandibular widths than normal, Chen et al. (2007), [13] Tricoveluri et al. (2013) [14] & Ponraj et al. (2016). [15] Musculature has been considered as a possible link in this close relationship between the transverse dimension and vertical facial morphology. Strong or thick mandibular elevator muscle in short face individuals might be the reason for increased dental arch width and alveolar arch width in hypodivergents. This muscular hyperfunction causes an increased mechanical loading of the jaws which in turn may cause an induction of sutural growth and bone apposition which then results in increased transverse growth of the jaws and bone bases for the dental arches. Benington, Gardener & Hunt (1999) evidenced that large masticatory muscles are associated with brachycephalism and vice versa. [16] Van Spronsen et al (1992) found that long‑faced subjects have significantly smaller masseter and medial pterygoid muscles than normal subjects. [17] Satiroglu, Arun & Isik (2005) [18] ultrasonographically measured masseter muscle thickness and found that individuals with thick masseter had a vertically shorter facial pattern and individuals with thin masseter had a long face.
Also the direction of mandibular growth is influenced by the tongue base position, as the anterior tongue pressure might influence on the rotation of mandibular corpus. Because of the lowered positioning of tongue, the balance between the tongue and buccinators muscle (buccinators mechanism) might be disturbed and this can be a reason for the arch constriction in maxilla. Mandible also constricts along with maxilla since maxillary and mandibular arches are mutual counterparts according to Enlows counterpart principle.
Conclusion
Maxillary and mandibular dental arch width (intercanine width, interpremolar width and intermolar width) were maximum in hypodivergents followed by normodivergents and minimum in hyperdivergents.
Maxillary and mandibular alveolar arch width (canine alveolar width, premolar alveolar width and molar alveolar width) were maximum in hypodivergents followed by normodivergents and minimum in hyperdivergents.
Since dental arch width and alveolar arch width were found to be associated with facial divergence; therefore, during orthodontic treatment, it is suggested to use individualized arch wires according to each patients pretreatment arch form and widths.
Limitations and Further Scope
The possible short-comings and limitations include errors in tracing, digitizing and measurements. Measurement accuracy is sensitive to human errors and is governed by sensitivity of measuring instruments. There were likely unavoidable magnification differences among different cephalometric films.
This study can be further carried out by dividing the samples into different sex group, so that further discussion of study can ease the clinicians to individualize the archwires among males and females for better treatment and results.
Source of Funding
None.
Conflict of Interest
None.
References
- R Mangla, N Singh, V Dua, P Padmanabhan, M Khanna. Evaluation of mandibular morphology in different facial types. Contemp Clin Dent 2011. [Google Scholar]
- TM Peterson, JD Rugh, JE Mciver. Mandibular rest position in subjects with high and low mandibular plane angles. Am J Orthod 1983. [Google Scholar]
- VJ Patel, AF Bhatia, SM Mahadevia, S Italia, M Vaghamsi. Dental arch form analysis in Gujarati males and females having normal occlusion. J Ind Orthod Soc 2012. [Google Scholar]
- RT Lee. Arch width and form: a review. Am J Orthod Dentofac Orthop 1999. [Google Scholar]
- JA Nasby, RJ Isaacson, FW Worms, TM Speidel. Orthodontic extractions and the facial skeletal pattern. Angle Orthod 1972. [Google Scholar]
- AK Khera, GK Singh, VP Sharma, A Singh. Relationship between dental arch dimensions and vertical facial morphology in class I subjects. J Ind Orthod Soc 2012. [Google Scholar]
- M Prasad, ST Kannampallil, AK Talapaneni, SA George, SK Shetty. Evaluation of arch width variations among different skeletal patterns in South Indian population. J Nat Sci 2013. [Google Scholar]
- C Grippaudo, B Oliva, AL Greco, S Sferra, R Deli. Relationship between vertical facial patterns and dental arch form in class II malocclusion. Progress in Orthod 2013. [Google Scholar]
- SS Jumani, G Erum. Correlation of vertical facial morphology and dental arch width in untreated Pakistani adults. Int J Dent Health Sci 2014. [Google Scholar]
- M Alghamdi, N Tashkandi. Relationship between Dental Arch Parameters and Mandibular Plane Angle. J Adv Med Dent Sci Res 2022. [Google Scholar]
- S Yamamoto, C Tanikawa, T Yamashiro. Morphologic variations in the craniofacial structures in Japanese adults and their relationship with sex differences. Am J Orthod Dentofac Orthop 2023. [Google Scholar]
- TE Christie. Cephalometric patterns of adult with normal occlusion. Angle Orthod 1977. [Google Scholar]
- F Chen, K Terada, L Wu, I Saito. Dental arch widths and mandibular-maxillary base width in Class III malocclusions with low, average and high MP-SN angles. Angle Orthod 2007. [Google Scholar]
- S Tricoveluri, JR Singh, N Rayapudi, A Karra, M Begum, PL Challa. Correlation of Masseter Muscle Thickness and Intermolar Width - An Ultrasonography Study. J Int Oral Health 2013. [Google Scholar]
- RR Ponraj, VA Korath. Relationship of Anterior Alveolar Dimensions with Mandibular Divergence in Class I Malocclusion - A Cephalometric Study. J Clin Diagn Res 2016. [Google Scholar]
- PC Benington, JE Gardener, NP Hunt. Masseter muscle volume measured using ultrasonography and its relationship with facial morphology. Eur J Orthod 1999. [Google Scholar]
- PH Van Spronsen, WA Weijs, J Valk, B Prahl-Andersen, V Ginkel. A comparison of jaw muscle cross-sections of long-face and normal adult. J Dent Res 1992. [Google Scholar]
- F Satiroglu, T Arun, F Isik. Comparative data on facial morphology and muscle thickness using ultrasonography. Eur J Orthod 2005. [Google Scholar]