Introduction
Class III malocclusion, also known as Angle's Class III, poses a significant challenge in treatment due to its combination of skeletal and dentoalveolar features. This malocclusion can manifest as mandibular skeletal protrusion, maxillary skeletal retrusion, a combination of both, or no abnormalities in either jaw. Dental issues such as proclined maxillary incisors and retroclined mandibular incisors may further complicate matters through dentoalveolar compensation.1, 2
Various treatment options are available for addressing Class III anomalies, depending on the specific jaw affected and the individual's growth period. These options include growth modification, orthodontic camouflage, orthognathic surgery, or a combination of these approaches.
This case report details the application of skeletal Class III orthodontic camouflage in an adult patient. The report outlines the diagnostic process and the careful consideration of therapeutic options before deciding on the extraction of the lower first premolar as part of the treatment plan.
Case Report
A 21years old female patient came with chief complaint of irregularly placed lower front teeth, general examination of patient showed mesomorphic body type with Athletic build, diagnosed with Angle’s Class III malocclusion on skeletal Class III base, vertical growth pattern, overjet of and overbite of 0 mm with proclined and protruded upper and lower incisors, with concave soft tissue profile and average nasolabial angle with competent lips. Figure 1 (a,b,c)
Intraoral assessment presented maxillary dental midline shifted to patients right by 1.5 and mandibular dental midline shifted to patients right by 1mm, crowding in upper lower anterior. There was no premature contact or functional displacement during jaw opening or closing. She also had good oral hygiene, healthy periodontal tissues, and a complete set of teeth. Figure 1 (d-h)
Figure 1
Pre treatment records, Extraoral photographs(a,b,c), Intraoral photographs (d-h), Pre treatment OPG (i), Pre treatment Lateral cephalogram (J)


Figure 3
Post treatment records, Extraoral photographs (a,b,c), Intraoral photographs (d-h), Hawley’s appliance for retention (i) Post treatment OPG (j), Post treatment Lateral cephalogram (k)
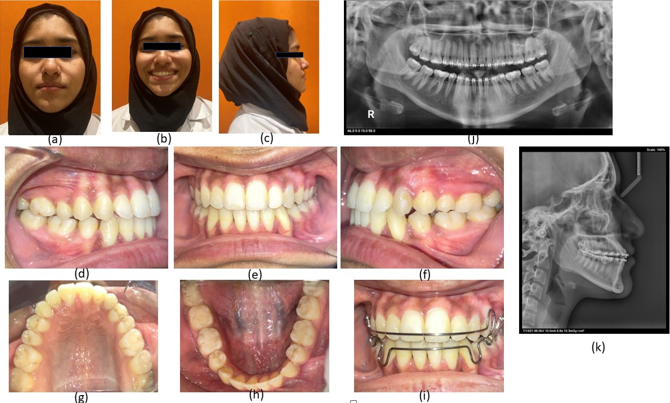
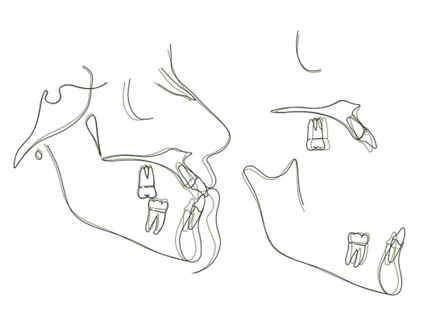
Table 1
Composite analysis skeletal analysis-sagittal
Table 2
Skeletal analysis –vertical
Table 3
Dento– alveolar analysis
Table 4
Soft tissue analysis
A lateral cephalometric analysis showed a Class III skeletal pattern with a prognathic maxilla and mandible with proclined incisors. The panoramic radiograph revealed a complete set of dentition with well erupted third molars. Figure 1 (i, j)
Initially, orthognathic surgery was proposed as the first treatment option, but the patient and her parents declined any surgical intervention. The second option involved addressing the issue with four premolar extractions (either upper and lower first or second premolars). While this approach could have corrected incisor proclination and crowding, it was deemed likely to worsen the patient's facial aesthetics by eliminating dental compensation, thereby accentuating the Class III profile.
The third alternative considered was orthodontic camouflage, achievable through the use of Class III elastics, distalization of the lower arch using Temporary Anchorage Devices (TADs), or mandibular first premolar extraction. However, the first two options were deemed unsuitable for this specific case. The use of Class III elastics was ruled out due to the need to correct upper incisor proclination, which could be exacerbated by their use. Similarly, lower arch distalization with TADs was considered impractical, especially given the unpredictability of the required lower distalization and the potential need for lower third molar extraction.
Consequently, the most reasonable option was determined to be orthodontic camouflage with extraction of the first mandibular premolar. This approach promised to normalize upper incisor inclination and correct mandibular crowding, leading to a predictable enhancement of facial aesthetics. Importantly, the biological cost associated with this option was deemed comparable to that of lower arch distalization. This approach gained preference from both the patient's parents and the orthodontists involved in the case.
The mandibular first premolar was extracted before bracket bonding. All teeth were bonded with brackets (0.22 slot; Ormco, Glendora, California) an MBT™ bracket prescription. Figure 2
Aligning and leveling of all teeth were achieved in 8 months by sequential use of NITI wires till a 0.019 × 0.25-in nickel-titanium archwire in the maxilla and a 0.017 × 0.025-in nickel titanium archwire in the mandible. Space closure on the mandibular teeth was completed in 10 months using an elastomeric chain and Class III elastics with a 0.019 × 0.025-in stainless-steel archwire. Some brackets were repositioned to improve occlusion and interdigitation. After 25 months of treatment, the fixed orthodontic appliance was removed. Post completion of treatment satisfactory results were achieved.Figure 3 (a-h)
In the retention phase, Hawley’s retention plates were given.Figure 3 (i)
Post treatment results
Skeletal: There was a normalization of the skeletal pattern with reduction of ANB to 2 degrees (-1 to 1º)because of backward movement of B point because of retraction of anteriors. No other significant changes were observed.FIGURE 3 (j,k)
Dental: Normalization of upper and lower incisors was observed with retraction of lower anteriors. Upper incisors were retracted by 2degree and 2mm and lower incisors were retracted by 2 degree (85 to 83). Normalization of interincisal angle to 135 degrees were also observed
Soft tissues: Harmonious soft tissue profile achieved by retraction of lower incisors, convex soft tissue profile with competent lips are achieved.A detailed pre and post cephalometric findings are presented in Table 1, Table 2, Table 3, Table 4 for detailed explanation and understanding of outcomes in orthodontic camouflage treatment in class III cases.
Appraisal of treatment: Patient was successfully treated by mandibular first premolar extractions for the reduction of arch length tooth material discrepancy and proclination of lower anteriors. The Angles Class III malocclusion was camouflaged by retraction of lower anteriors. Deep bite and overjet were also achieved to almost normal relationship, currently the patient has class I incisor and canine relationship with molars in therapeutic class III relationship. Figure 4
Discussion
Camouflage treatment can be an alternative for patients with mild to moderate Class III malocclusion and an acceptable facial profile. 3 Studies have shown that camouflage treatment in moderate skeletal Class III malocclusion provides long-term stability and satisfactory outcomes.4 Changes in skeletal, dental, and soft tissue can be camouflaged without undesirable effects on the periodontium, such as gingival recessions. Therefore, proper diagnosis and realistic treatment outcomes should be made by the orthodontist in collaboration with the patient.5
In this particular case, the patient opted against orthognathic surgery and chose a camouflage treatment that involved the extraction of the mandibular first premolars. Initially, the patient presented with a 0mm overjet and overbite on the central incisors, and there was sufficient thickness in the mandibular symphysis for the retraction of the mandibular incisors. Additionally, the patient exhibited moderate crowding, and the spaces created by the extractions were utilized to alleviate the crowding and retract the anterior teeth in the mandible.
Throughout the treatment, a deliberate effort was made to maintain a Class III molar relationship while achieving a Class I incisor and canine relationship. This strategic decision to preserve the Class III molar relationship helped avoid the necessity for additional dental extractions in pursuit of a Class I molar relationship. This specific type of occlusion, characterized by the retention of the Class III molar relationship, is commonly referred to as therapeutic Class III occlusion. Previous studies have shown that therapeutic Class III occlusion was viable with good occlusal stability and periodontal health after 13–14 years of follow-up.6 Another study also showed stability after three years of follow-up with a Class I canine and Class III molar relationships.7
This orthodontic treatment approach is unique due to:
Individualized Plan: Thorough consideration of the patient's skeletal, dental features, and preferences resulted in a tailored treatment plan, emphasizing unique clinical and extraclinical factors.
Camouflage Treatment: Choosing orthodontic camouflage for a non-growing patient with Class III malocclusion distinguishes this case. This strategy involves masking skeletal discrepancies through dental movements, avoiding surgery or extensive premolar extractions for satisfactory functional occlusion and aesthetics.
Preserved Class III Molar Relationship: The decision to maintain the Class III molar relationship avoids additional dental extractions for a Class I relationship, showcasing a strategic and conservative orthodontic philosophy.
Successful Camouflage Techniques: The case shows successful execution of camouflage techniques, including mandibular first premolar extraction, aligning and leveling with sequential NITI wires, and space closure with elastomeric chains and Class III elastics. The detailed description contributes to the case's uniqueness.
Long-Term Stability Considerations: The case alludes to studies indicating long-term stability of therapeutic Class III occlusion, emphasizing the importance of lasting outcomes in the patient's occlusion and periodontal health.
Lack of Guidelines Acknowledgment: Recognizing the absence of established guidelines for borderline class III orthodontic cases emphasizes the need for personalized treatment strategies, relying on clinical judgment and expertise.
Conclusion
As of the present, there are no established guidelines to assist orthodontists in navigating the decision-making process for borderline orthodontic cases. The provided case report illustrates that the selection of an effective treatment plan must consider numerous clinical and extra clinical factors, ultimately aiming for orthodontic excellence by tailoring the approach to each patient's unique needs.
This case highlights that individuals with mild to moderate skeletal Class III malocclusions have the option of orthodontic camouflage treatment as an alternative to enhance both functional occlusion and aesthetics. Achieving satisfactory results in such cases requires a thorough diagnosis, meticulous treatment planning, and the careful execution of the chosen approach. Additionally, patient cooperation is crucial throughout the treatment process to ensure successful outcomes. The absence of one-size-fits-all guidelines emphasizes the importance of a personalized treatment strategy for borderline Angles class III orthodontic cases.