Introduction
Ectopic eruption is a disturbance in which the tooth does not follow its usual course. In this case, the presence of a mesiodens has caused the central incisor to take a deviated path. Another ectopic eruption was noticed in upper left second premolar which erupted palatally to the main arch. This article presents the course of treatment followed after extraction of these ectopically erupted and supernumerary teeth. Their management included closure of the space created after their removal by mesialisation of the arch in two segments. It was successfully managed by using the mini implants for absolute anchorage and friction less mechanics.
Case Report
A 15 year old male GP presented with the chief complaint of irregularly placed upper front teeth Extraoral examination shows convex facial profile, mesocephalic head shape and leptoprosopic facial form, no gross asymmetry of face, average nasolabial angle, shallow mentolabial sulcus and competent lips. 1
Intraoral findings include Molar relation Class I on right side and End on relation on left side, Canine relation class I on the right side and class III on left side. Presence of mesiodens between 11 and 21. Presence of palatally placed and fractured 25. Overjet of 4 mm and overbite of 5 mm. Mesiolabial rotation of 14, 21, 24, Distolabial rotation of 35, 44. Not recordable upper and lower dental midlines. 2, 3, 4
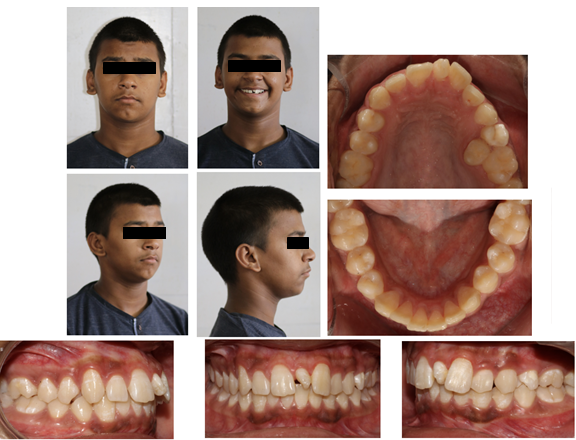
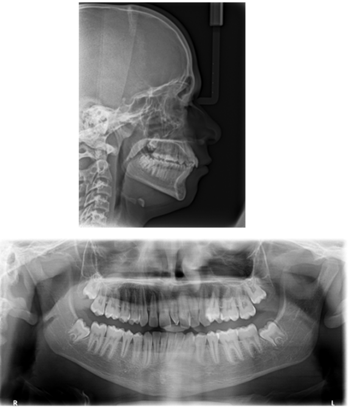
Cephalometric findings showed skeletal Class I jaw bases with orthognathic maxilla and mandible and normodivergent growth pattern, Normally inclined upper and slightly proclined lower incisors.
Model analysis reveals arch perimeter excess by 1.5 mm in upper arch and 1 mm tooth material excess in lower arch.
Treatment Objective
Leveling and aligning the teeth in both the arches
Correction of rotations
Correction of spacing and crowding
To establish proper overjet and overbite
To establish proper occlusion and midline
Treatment progress
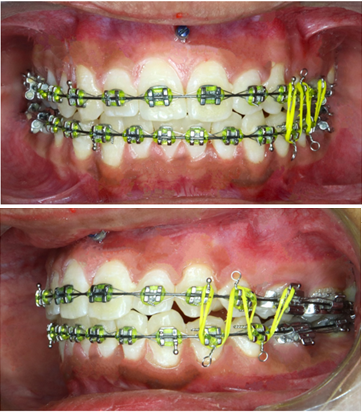
Extraction of mesiodens and blocked out 25 with fracture was done. Initial leveling and alignment started in following sequence for both the arches - 0.014′′ NiTi, 0.016′′ NiTi, 0.018′′ NiTi, 0.018′′ SS and 16×22 SS for 6 months. After this, mini implants were placed between 11 and 21. Sectional T-loop was given with absolute anchorage for mesialisation of 22 and 23. Simultaneously, arch was consolidated from 16 to 21. This was continued for 4 months. After completion of mesialisation, T-loop was removed. Now for mesialisation of 25 and 26, Cherry loop was fabricated using 17×25′′ TMA wire that took 3 months to complete. Arch wires were updated to rectangular SS wires. 5, 6, 7, 8, 9
Class II elastics were given on right side and class III elastics were given on left side for next 4 months. To achieve good cuspal interdigitation and settling elastics were given for 3 months.


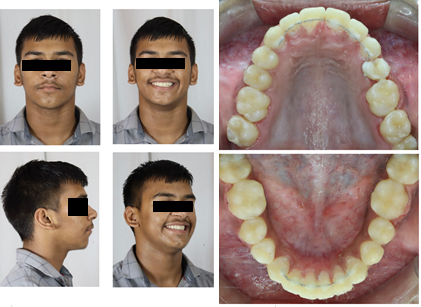
Treatment Result
Treatment objectives were fulfilled with establishment of overjet and overbite of 2mm. Class I molar on right side and class II on left side. Canine relation class I on both the sides were appreciable. There was complete space closure in both the arches along with proper alignment.
The post treatment cephalometric evaluation showed that there was increase in following angles : SNA by 1°, SNB by 2°, FMA by 4°, UI-SN by 3° and decrease in IMPA by 5 °. All variations are within normal range.

Discussion
Technology advancement has contributed significantly to the field of treatment planning in dentistry and Orthodontics. Application of mini implants in modern dentistry has revolutionized treatment approaches to reach ideal treatment results. One such case has been presented that emphasizes on space closure by means of arch mesialisation in two segments. Mesial movment of whole arch from left side may cause anchorage loss, so two step mesialisation was planned. Firstly the space created by supernumerary teeth was closed till canine by segmental T-Loop using absolute anchorage. Remaining posterior segment was mesialised by using loop mechanics. Loss of anchorage is the foremost concern in such cases, but with the help of mini implants it was done with predictable results. If mesialisation was not planned in this case, there could have been chances of not achieving proper molar and canine relation. Patient is expected to have stable results as the treament was done in early stages of growth.10, 11, 12, 13
Conclusion
Innovative application of Temporary Anchorage Devices could simplify the modification of iatrogenically skewed dental arches with desirable aesthetics. Using these have provided a more predictable and less invasive treatment results compared to other compelling treatment plan alternative. The planned treatment was executed with absolute anchorage without any complication. The overall treatment time was 20 months. The desired objectives of smile and facial esthetics, functional occlusion and stability were achieved.