Introduction
Before lateral cephalographs were widely used, soft tissue profiles were examined. In order to show racial differences and evolutionary developments towards the end of the 18th century, Camper (1794) 1 introduced a line and an angle that were later named in his honour in anthropology. Retzius categorised human races as orthognathic or prognathic in the early 19th century (Neger, 1959), 2 and Case (1921) 3 identified specific areas of the human face that underwent the most significant changes following orthodontic treatment. The invention of the lateral cephalograph by Broadbent4 and Hofrath 4 in 1931, with its representation of skeletal and dental structures, signalled the start of a new branch of orthodontic diagnostics. In spite of profile photos living a "shadow" existence in the following years, new analysis techniques were still being developed. The definition of the facial thirds by Schwarz 5 (1961) and descriptions of the profile using the jaw profile field (Schwarz, 1958), 6 the H line (Holdaway, 1984), 7 or the angle of facial convexity (Muzj, 1956; Burstone, 1958; Subtelny and Rochester, 1959) 8, 9, 10 were also made. Individual structures such as the lips or nose were also examined (lip profile analyses according to Korkhaus (1939), Schwarz (1958), or Ricketts (1988).11, 6, 12
Computer-assisted analyses of facial photographs have drawn more attention recently. Edler et al. (2001, 2003, 2004) 13, 14, 15 described how to use en-face photographs, particularly those of the mandibular region, to identify facial asymmetries. They emphasised the benefit of non-invasiveness in comparison to dental tomographs. According to a method Schwarz (1958) 6 developed to describe an average or 'biomet' face based on a jaw professional field, skeletal Class II and Class III subjects were significantly more likely to deviate from the facial type. Muzj (1956)8 similarly found significant deviations from the normal profile defined by the frontal-facial angle in skeletal Class II and Class III malocclusions, although he did not compare them to any measures from a lateral cephalographs examination.
It is unclear if the skeleton Class can be determined from a lateral (profile) photograph and which method of angle determination or analysis is most appropriate. In Orthodontics, the usefulness of an analytical method hinges on the use of ideas and structures that are mostly unaffected by growth. The "facial angle of convexity excluding the nose," also known as the "facial contour angle," is frequently described in the literature as stable (Subtelny, 1961; Mauchamp and Sassouni, 1973; Rakosi, 1979; Bishara et al., 1985, 1998). 16, 17, 18, 19, 20 However, a cross-sectional study by Pelton and Elsasser (1955)26 revealed that this angle reduced throughout the growth process, with the reduction being more pronounced in girls than in boys. Long-term observations on patients with a normal profile and a neutral occlusion were published by Subtelny and Rochester (1959). 10 Mauchamp and Sassouni (1973), 17 and Bishara et al. (1985, 1998) 19, 20 Although they noticed a slight rise in the angle of convexity, they believed that this angle was, on the whole, stable. Riolo et al. (1986) 21 found no influence on the angle of convexity in their relationship between body weight and the thickness of the soft tissues.
The angle of convexity seems to be the most appropriate parameter in this regard, but different authors have defined it differently. For example, some authors use the soft tissue glabella point (Gl′; Burstone, 1958; 9 Mauchamp and Sassouni, 1973, 17 Chaconas and Bartroff, 1975; 22 Bishara et al., 1985, 1998), 4, 11, 6, 12, 5, 7, 8, 9, 10, 13, 14, 15, 23, 24, 25, 26, 16, 17, 18, 19), while others use a frontal point (Fr; Muzj, 1982) 27 similar to the trichion point, an NS point defined on the lateral cephalographs by extending the Ba–N line (Subtelny,1961), or an N′ point located at the bottom of the depression above the nose (Phillips et al., 1984; Satravaha and Schlegel,1987; Zylinski et al.,1992; Ngan et al.,1996; Ruf and Pancherz, 1999) 28, 4, 11, 6, 12, 5, 7, 8, 9, 10, 13, 14, 15, 23, 24, 25, 26, 16, 17, 18, 19, 20, 29, 21, 27, 22, 30 as cranial reference points. Figure 1 depicts the data points used in the current study for comparison. Depending on the study, the central reference point was either the subnasal point (Sn) at the junction of the nasal columella and the upper lip (Pelton and Elsasser, 1955;, 29 Burstone, 1958; 9 Subtelny and Rochester, 1959; 10 Mauchamp and Sassouni, 1973, 17 Rakosi, 1979;, 18 Muzj, 1982, 27 Satravaha and Schlegel, 1987; 31 Zylinski et al., 1992; 32 Ngan et al., 1996, 33 Ruf and Pancherz, 1999) 34 or the deepest point of the concavity of the upper lip described as A′ (Bowker and Meredith, 1959) 35 or superior labial sulcus (SLs; Phillips et al., 1984; 30 Bishara et al., 1985, 1998). 4, 11, 6, 12, 5, 7, 8, 9, 10, 13, 14, 15, 23, 24, 25, 26, 16, 17, 18, 19 The caudal reference point is sometimes the soft tissue gnathion point (Gn ′; Muzj, 1956) 8, but more frequently the soft tissue pogonion point (Pog ′; Pelton and Elsasser, 1955; 29 Burstone, 1958; 9 Subtelny and Rochester, 1959; 10 Merrifi eld, 1966; 36 Mauchamp and Sassouni, 1973; 17 Rakosi, 1979; 18 Bishara et al., 1985, 1998, 19, 4 Satravaha and Schlegel, 1987; Zylinski et al., 1992; Ngan et al., 1996; Ruf and Pancherz, 1999). 30, 31, 32, 33, 34 Given the broad spectrum of different approaches regarding the profile angle, another question is raised whether it is possible to determine the skeletal Class from a lateral (profile) photograph and which reference point of the angle of convexity is most suitable for this purpose.
Materials and Methods
Retrospective analysis of patient information from 60 patients in orthodontics department was done. A lateral cephalogram and a profile photograph of high quality taken on the same day met the inclusion requirements. The Wits value according to Jacobson (1975) 37 was calculated using the lateral cephalograph to categorise the patients as skeletal Classes I, II, or III. Skeletal Class I values for male patients ranged from - 1 to + 2 mm, whereas the range for female patients was 0 to + 2 mm. According to Jacobson (1975; Table 1), larger values were classified as skeletal Class II and smaller values as skeletal Class III.
Table 1
lassification according to Jacobson (1975). Wits values; including population sizes and sex distributions as well as the means and standard deviation for age
|
Wits |
N |
Male/Female |
Age (years) |
|
Class I |
20 |
5/15 |
13.3 ±1.42 |
|
Class II |
20 |
9/11 |
13.85 ± 1.27 |
|
Class III |
20 |
10/10 |
13.60 ± 1.23 |
Table 2
he distribution of males and females for the three skeletal groups
Table 3
Results for angles A ′ N ′ B ′ , A ′ OrB ′ (=POrA ′ – POrB ′ ), N ′ SnPog ′ , N ′ A ′ Pog ′ , TrSnPog ′ , TrA ′ Pog ′ , Gl ′ SnPog ′ , and Gl ′ A ′ Pog ′ for the respective skeletal Classes including the 95 per cent confidence intervals
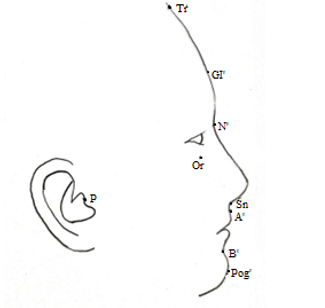
The profile photograph was used to mark the following soft tissue measuring points: trichion (Tr), glabella (Gl ′), nasion (N ′), subnasal point (Sn), superior labial sulcus (SLs or A ′), inferior labial sulcus (ILs or B ′), pogonion (Pog ′), porion (P), and orbital (Or) (Figure 1). Based on these points, the following version of the angle of convexity were measured: N ′ SnPog ′, N ′ A ′ Pog ′, TrSnPog ′ , TrA ′ Pog ′ , Gl ′ SnPog ′ , and Gl ′ A ′ Pog ′ . A ′ OrB ′ (=POrA ′ – POrB ′) and A ′ N ′ B ′ were also measured for comparison. A deviation from the normal distribution could not be determined for the individual classes and angles based on a Kolmogorov – Smirnov test at the 0.05 level. It was therefore possible to obtain statistical comparison using a two-sided t -test for independent samples
Results
hows the distribution of males and females for the three skeletal groups. Table 3 shows the results for the three skeletal groups and the various angles and the P values obtained with the t -test. The highly significant differences ( P < 0.001) between all angles for Class II and Class III and almost all angles for Class I and Class II are evident, the only exception in the latter case being A’OrB′, where the level of significance was only P >0.05. The differences between Class I and Class III were statistically much less significant, A′N′B′ and N′A′Pog′ were the two angles with level of significance p>0.05.
The last three columns show the P values obtained by statistical analysis using the t -test for unconnected samples for intergroup comparisons.
Discussion
This study looked at whether it was possible to identify the skeletal Class from a lateral (profile) photograph and which angle would be most useful.
The literature has hardly ever discussed variations in soft tissue profile angles for the various skeletal Classes. According to Muzj (1956), 8 the frontal-facial angle (also known as the faciocranial angle, Fr - Sn - Gn ′) should be between 174 and 177 degrees. Less than 173 degrees and more than 179 degrees were considered "extranormal" because they represented skeletal Class II and Class III, respectively. He defined the ranges of 173 - 174 degrees and 177.5 - 179 degrees as "paranormal." The symmetry of the two sides of the angle in relation to its bisector, which runs along the mandibular base, was given much more importance by that author. If the symmetry was compromised, it was thought that there was an anomaly or disharmony that needed to be addressed (Muzj 1956, 1982, 1983, 1985a, b, 1988) 8, 27, 38, 39, 40, 41 Since the mandibular base measured on a lateral cephalograph was used to construct Muzj's frontal-facial angle, it was not possible to compare these values to those obtained in the current study. From there, it is determined that the frontal point, Fr, is the highest and most anterior point of the cerebral cranium. Gn is used as a reference causally. According to the soft tissue profile points.
Among the angles investigated in the current investigation, TrSnPog ′ was the most similar to Muzj's description. The values discovered in this study for Classes I and II were significantly below those that Muzj reported. Contrarily, one would have anticipated higher values given that the Pog ′ point used was situated more anteriorly than Muzj's Gn ′ point. The Fr point used by Muzj and the trichion used in the present study were not the same, which could be one explanation. However, based on Muzj's descriptions from 1956 and 1982, 8, 27, 38, 39, 40, 41 the Fr point is most likely situated close to the hairline. According to this study N ′ SnPog ′, GlA ′ Pog ′, TrA ′ Pog ′, Tr Sn Pog’, GI’ Sn Pog’ are the angles of convexity best suited for skeletal class determination, similar to a study by Godt in which he concluded that N ′ SnPog ′, GlA ′ Pog ′, TrA ′ Pog were the angles most suited for skeletal class determination.42
Although there was a significant age gap between the subjects (Muzj developed his method primarily with adult subjects, whereas the mean age in this study was 13.6 years), this would not account for the differences observed. Although adolescence has been associated with a slight increase in the angle of convexity, a long-term comparison would still need to be based on the supposition that the proportions are stable (Subtelny and Rochester, 1959; 10 Bishara et al. 4, 19
Other authors have examined only subjects with a "fair face" (Burstone, 1958; 9 Zylinski et al., 1992) 32 orthoocclusion (Mauchamp and Sassouni, 1973; 17 Bishara et al., 1985, 1998,) 4, 19 or skeletal Class I (Subtelny and Rochester, 1959,) 10 or they have only reported mean values for the angle of convexity and its variants. As a result, only the measurements for skeletal Class I in the current study can be used to compare the results. Based on the N′, Sn, and Pog′ points, Satravaha and Schlegel (1987) 31 and Zylinski et al. (1992) 32 calculated the angle of convexity.
Therefore, it seems possible to make a comparison with the corresponding angle in the current subject population. The mean value for children aged 5 to 10 years with a "handsome" face, a "harmonious profi le," competent lips, and a "normal" overbite and overjet was 163.3 degrees, ranging between the extremes of 154.2 and 170.9 degrees, according to Zylinski et al. (1992; 32 the corresponding values for adults aged 20 to 32 years meeting the same description were 166 degrees (153.4 - 175.9 degrees). The results of those authors would be confirmed by the mean value of this study, which is 155.5 degrees, and the mean age of 13.7 years, which both fall within this range and lead to the assumption of a slight growth-related enlargement (Subtelny and Rochester, 1959; 10 Mauchamp and Sassouni, 1973). 17 For their angular measurements, Subtelny and Rochester (1959) 10 used the NS point, which is slightly farther cranially than the N ′ point. They obtained mean values of 161.4 degrees for male and 161.0 degrees for female 14-year-olds (skeletal Class I, no orthodontic treatment). Pelton and Elsasser 29 reported in 1955 that over 8400 people participated in a cross-sectional study. Mean values for the subjects ranged from 162 to 166.5 degrees. In 1958, Burstone 9 discovered a mean GlSnPog ′ angle of (Extremes: 155.5 and 179.5 degrees) in young people adults who put on a "good face." Sassouni and Mauchamp (1973) 168 degrees for men and 165 degrees for women have been recorded.for subjects 13.5 years of age (female). The findings of this study largely support these conclusions. Similar to this was the case for the studies of Bishara et al. 19, 4 who reported GIA′ Pog ′ angles between 166.9 and 168.8 degrees for boys who have a good occlusion.