Introduction
An impacted tooth is one that fails to erupt into the oral cavity within the expected time. The frequency of maxillary central incisor impaction has been found in the range of 0.006% to 0.2%. 1 The dilaceration is characterized by an angulation in the crown and root of the tooth. This is often related to the trauma from the primary central incisors during the early developmental stages of the permanent central incisors.2
Orthodontic correction of severely dilacerated deflected impacted maxillary incisors is challenging due to its limiting factors like ankylosis, position of teeth, root resorption, time of treatment, successful outcome, multidisciplinary approach, patient cooperation, long duration and follow-up of treatment etc. (3-8). Delay in orthodontic and surgical intervention will result in unnecessary difficulties in aligning the tooth in the arch.3
Case Report
A 10-year-old boy reported to the Department of Orthodontics, Modern Dental College and Research Centre, Indore, India, with a chief complaint of non-eruption of front two teeth giving ugly look and hampered facial aesthetics. Patient had a history of trauma 4 years ago with the avulsion of deciduous maxillary central incisors. No relevant past medical history.4, 5, 6
Diagnosis
The clinical examination revealed a mesoprosopic facial form and a convex facial profile and presence of good facial balance. An intraoral examination revealed the mixed dentition with Angle's Class I Molar relation bilaterally with two missing maxillary permanent central incisors [Figure 1]. An intraoral periapical radiograph of upper anterior region demonstrated impacted permanent both maxillary central incisors. [Figure 2]. To confirm the position and morphology of impacted teeth an occlusal radiograph [Figure 3] and Panoramic (orthopantomogram or OPG) were taken [Figure 4]. Table showing Comparison of Cephalometric analysis and its inference showing changes in pre-treatment and post treatment.(Table 1) This established a diagnosis of bilaterally impacted, dilacerated and deflected maxillary central incisors. It was decided to orthodontically align the incisors. The CBCT of maxilla was taken to further confirm the root dilacerations of inverted maxillary incisors and its 3-dimensional position in maxilla. Maxillary central incisors were seen inverted with cingulum facing labially and also touching the nasal floor with crown root angulation nearing right angle. [Figure 5]
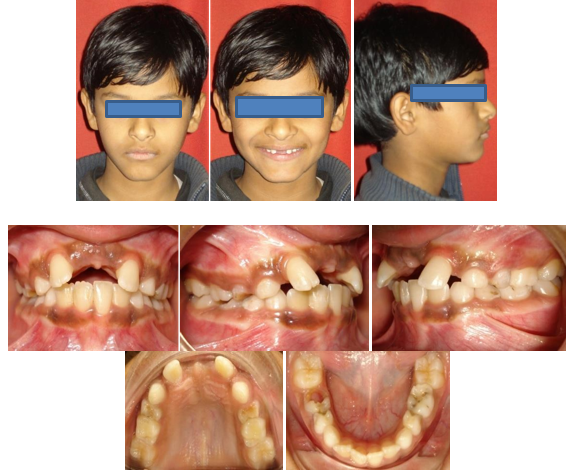


Figure 4
Pre-treatment OPG and lateral cephalogram showing inverted maxillary central incisors, mixed dentition and erupting canines and premolars.

Figure 5
CBCT image of maxilla showing both maxillary incisors dilacerated inverted and deflected to nasal floor with cingulum facing labially.

Table 1
Table showing comparison of cephalometric analysisand its inference showing changes in pre-treatment and post treatment.



Treatment Planning and Progress
Class II elastics were used for settling the occlusion. (Figure 13). Once the desired occlusion was achieved then the debonding was done and fixed retainers were delivered to the patient. (Figure 14). The follow up of patient was done at regular intervals. Latest records collected at the stage of 10 years follow up. (Figure 15).8
Figure 6
Surgical exposure of central incisors and attachment of lingual buttons to the exposed crown of maxillary central incisors.

Figure 7
Modified TPA in place with anterior hooks and anterior acrylic extension to prevent tissue injury from ligature wires





Figure 12
Intra-oral and extra-oral photographs, OPG and lateral cephalogram after 10 years follow up

Figure 13
Superimpositions of pre-treatment and post treatment cephalograms showing changes of incisal inclinations.

Alternate treatment plan option-
Extraction of impacted teeth and replacement with dental implants.
Creation of space for impacted tooth, surgical crown exposure and orthodontic traction of the impacted central incisor.
Extraction of impacted central incisor and temporary restoration with removable prosthetic denture, followed by a permanent restoration with a bridge or an implant when growth ceases.
Extraction of impacted central incisor and closure of the space, converting the lateral incisor into central incisor with subsequent prosthetic restoration.
Discussion
Impacted maxillary permanent central incisor due to dilacerations is rarely seen and has serious impact on aesthetics, phonetics, mastication, and psychology in young patients. Orthodontic treatment of impacted and dilacerated maxillary anterior teeth is one of the most challenging task for orthodontists due to its limiting factor like position of the impacted tooth, degree of root completion, direction of impacted teeth, degree of dilacerations, and the presence of space for the impacted teeth. This case was challenging as both the maxillary central incisors had dilacerations and roots were deflected labially pushed to floor of nose, with crown root angulation nearing right angle. Limitation of this case was that ideal tip torque could not be achieved as there was fear of fenestration by dilacerated root. A ten-year follow-up of the stability and periodontal health showed that the tooth placed in the occlusion maintained both aesthetics and function. This case report thus establishes that dilacerated inverted teeth can be successfully aligned with early intervention and multidisciplinary approach without root resorption.
Conclusion
Bilateral impaction, dilacerations and internal deflection of both maxillary permanent central incisors is a relatively rare phenomenon but when present they pose a multitude of diagnostic, prognostic, and management challenges. To reach a definitive diagnosis and improve treatment planning, the role of latest imaging tools such as CBCT is indispensable along with essential diagnostic aids. Treatment should commence as early as possible and comprises surgical exposure followed by orthodontic traction and tooth alignment in the dental arch. For successful management, a multidisciplinary approach and a high level of cooperation from the patient are required.