Introduction
Class III malocclusion has a 3.4% incidence and thus its prevalence varies among different ethnic groups. 1, 2, 3 The severity of Class III malocclusion and the patient's age are the determining factors in its treatment. Orthognathic surgery is the best option for severe cases on the other hand, orthodontic camouflage can be attempted in mild to moderate cases. 4, 5 Camouflage treatment can be attempted with two approaches: In first approach extraction of either lower first premolar or lower incisor; In the second approach mandibular molar distalisation can be done with buccal shelf screw after third molar extraction.
An efficient orthodontist can utilize the range of treatment modalities, such as myofunctional, orthopaedic, orthodontic, or surgical treatment, to the maximum extent possible, depending on the patient’s growth potential and the exact assessment of the malocclusion, both skeletally and dentally. Treatment of skeletal malocclusions resulting from discrepancy in the mandible, maxilla, or both is more crucial than for dental malocclusions.
Skeletal Class III malocclusion commonly having anomaly in size and/ or position of the jaws in sagittal plane. The malocclusion occurs due to retrognathic maxilla and prognathic mandible or combination of either of the two. These cases constantly present concave or straight facial profile depending on the severity of the malocclusion, prominent chin, and dentally with an anterior crossbite.
In orthodontics, camouflage therapy involves moving teeth in relation to their supporting basal bone to make up for any disparity in the jaw. Proclination of the maxillary incisors and retroclination of the mandibular incisors are typically used in the camouflage technique to treat Class III malocclusion in order to correct anterior crossbite. The orthodontist must always provide the appropriate appliance to the patients at the appropriate time. If the child's growing phase is not used to rectify the developing malocclusion, it will also result in a more complex malocclusion that can only be addressed surgically. Because of the sagittal aspect of the envelope of discrepancy, the correction of a skeletal Class III malocclusion with a maxillary defect is less likely to be successful than a mandibular defect.
It was also established that older age causes skeletal Class III malocclusion to worsen much more, making early repair crucial. With the aid of tooth compensation, camouflage therapy improves aesthetics in mild to moderate skeletal Class III cases by concealing skeletal issues and achieving good occlusion and function.
For individuals who do not want surgery, the sole choice in borderline cases is camouflage treatment. ANB angle and facial aesthetics can be reduced using Class III camouflage treatment, with little to no change in the vertical dimension of occlusion. Orthodontic therapy alone can be an effective treatment for adult Class III malocclusion situations with proper selection and advice.
This case report aims to present orthodontic camouflage treatment using buccal shelf mini screws in a case with Class III malocclusion. This case report documents the clinical operation of an adult skeletal and dental Class III malocclusion complicated with anterior and posterior crossbite, and midline shifted to left. Conservative treatment approach can be taken to treat this case and acceptable result can be achieved.
Case Presentation
A 23-year-old patient reported with following complaint: Protruded chin, spacing between upper front teeth, forwardly placed upper front teeth, difficulty in chewing food with poor facial appearance and midline shift towards left. There was no contributory medical and dental history.
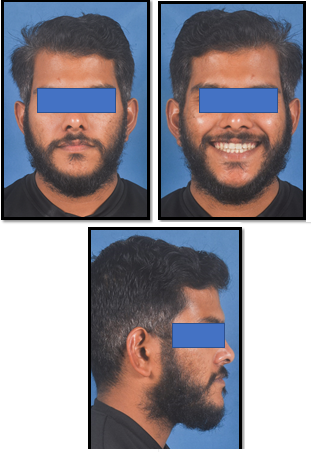
On clinical examination the case was mesoproscopic with concave profile, negative lip-step, anterior divergence, conclave profile, well-proportioned face with competent lips. (Figure 1)
On smile analysis showed symmetrical smile with a flat smile arc, low lip lin, and canting of the occlusal plane or buccal corridor was seen on smiling.
On intra-oral examination all the compliments of teeth present, Angle Class III molar relationship bilaterally, mild spacing in maxillary arch, the lower arch showed a very mild degree of crowding, anterior and posterior crossbite present, lower dental midline shift toward left side by 4 mm. (Figure 2)
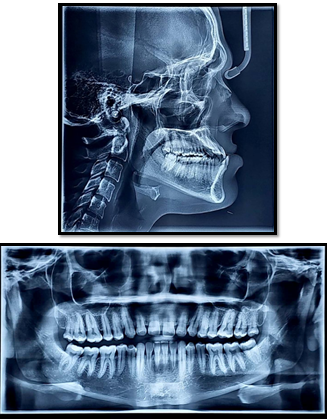
Cephalometric examination and analysis showed the skeletal Class III tendency, with retrognathic maxilla and prognathic mandible, horizontal mandibular plane angle with proclined and protruded maxillary incisors and upright mandibular incisors. (Table 1)
Panoramic radiograph showed all compliments of teeth including all third molars. No abnormal findings were noted.
Table 1
Cephalometric analysis


Treatment Objectives
To correct the prognathic mandible.
To correct the anterior crossbite.
To correct the posterior crossbite.
To correct the spacing in between upper anteriors and crowding in relation to the lower anteriors.
To achieve ideal overjet, overbite, and obtain Class I incisor relation
To correct the protrusive lower lip
To maintain the straight facial profile of the patient
To achieve pleasing esthetics smile.
Treatment alternatives
Orthognathic surgery was the first treatment plan recommended for our patient to reduce mandibular protrusion. The second treatment alternative was the distalization of the mandibular teeth using buccal shelf screws for camouflage treatment. Since the patient did not accept orthognathic surgery, it was decided to distalize mandibular teeth using bone screws.
Treatment plan
Fixed mechanotherapy using MBT 0.022 inch slot was planned (Bonding from 7-7).
The anterior crossbite was planned to be corrected by opening the bite with the help of bite block, and retroclination of lower anteriors by means of placement of continuous elastomeric chain, using the buccal shelf screws and posterior crossbite corrected with wide archform, After the desired amount of overjet was achieved by leveling and alignment of the upper teeth, following which the settling of posterior occlusion, leveling, and alignment of the lower teeth would be done. The spacing would later be closed in the upper arches along with midline correction.
Retention plan
The retention protocol was fixed retainers from 3-3 to Lingual bonded retainers in the upper and lower arches along with Hawleys plate in order to avoid any relapse, allow for teeth settling, maintain the arch.
Treatment progress
Phase I: Initial alignment and levelling of upper and lower teeth was achieved using 0.014”, 0.016’’, 16×22’’ nickel titanium (NiTi) wires and later on with 17×25 NiTi wires and subsequent wires, 19x25’’ NiTi and 19x25’’SS wires. The lower third molors were planned for extraction.
Phase II: The lower arch was consolidated and after 3 months, 2x12-mm Buccal Shelf stainless steel screw (Favanchor, India) were placed bilaterally on the buccal shelf region.
150-g of force was applied bilaterally from the miniscrews to the lower teeth using a closed elastomeric chain (Orthosystems, India). Following 4 months of force application, distalization of the mandibular arch was completed. No interproximal reduction was performed in the lower arch. The fixed appliances were removed 16 months after the beginning of treatment. (Figure 4, Figure 5)
Phase III: Final finishing and detailing were done using 0.016 NiTi archwire and with M-shaped settling elastics.



Treatment Results
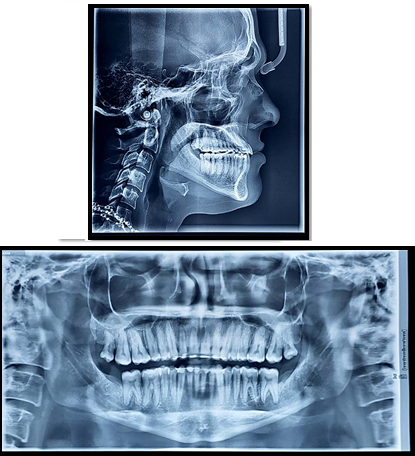
It was observed that the patient’s soft tissue profile improved. Anterior and posterior crossbite was corrected, and lower arch crowding was resolved. Angle’s Class I canine and class I molar relationship was obtained. Adequate root parallelism was achieved and root resorption did not see. The patient’s chief complaint of anterior crossbite was successfully relieved and normal overjet and overbite and a stable occlusion with good intercuspation was achieved. The patient’s profile was dramatically improved from concave to straight profile with very pleasing aesthetics. (Figure 6, Figure 7, Figure 8)
Discussion
Comprehensive orthodontic treatment in an adult patient aims to produce a Class I molar and canine relationship compensating for the underlying skeletal discrepancy. The treatment decision for Class III malocclusion depends on the clinical evaluation, cephalometric values, sagittal and vertical discrepancy, dentoalveolar components and facial esthetcis. Patients with an orthognathic profile in centric relation and Angle’s class I molar relation, crowding in upper and lower arch and functional shift are the good candidates for camouflage treatment. However, treating Class III malocclusion with orthodontic camouflage may lead to increased proclination of the maxillary incisors and recroclination of mandibular incisors, especially if there is an underlying skeletal Class III tendency.6
The biomechanics of Class III elastics focuses on flaring of the maxillary incisors, retroclination of the lower incisors, extrusion of the upper molars, posterior rotation of the mandible, and an increase in vertical dimension. 7, 8 Here in this case, extrusion and mesialisation of maxillary molars would have caused open bite tendency and increased vertical height.
Miniscrews eliminates the need for patient co-operation and do not induce proclination of the upper incisors or extrusion of the upper molars.9 To avoid effects of Class III elastics, we implemented miniscrew-supported distalization in this case. In literature, molar distalization amounts with the aid of mini-implants or mini-plates varies between 2-6 mm. Sugawara et al. achieved mandibular molar distalization of 3.5 mm at the crown level and 1.8 mm at the root level, and the average amount of relapse was 0.3 mm at both the crown and root apex levels.10 Poletti et al. 4 reported 4mm of molar distalization with a tipping of 10°.11
Mini-screws and mini-implants have been inserted into different areas for anchorage. Some authors placed the mini-impant in the anterior border of ramus for the distaliastion of mandibular arch. 10, 11 A limiting factor for buccal shelf crews placed in the interradicular region is inadequate distance between the tooth roots. 12 Chung et al. in his study inserted a C-shaped mini-implant into the maxillary molar area for using Class III elastic through this implant. 13 Later, Following the method of Chung et al. he strategically inserted C-implants between the mandibular first molar and second premolar. This method facilitated distalisation of second molars using a sliding jig connected to the main archwire that transferred the elastic forces to second molars from the mini-screws. 14 In this case, we positioned the screws distal to second molars in the buccal shelf region for distalisation of the mandibular arch. Miniplates and extra alveolar screws (such as buccal shelf) can be employed in situations where skeletal anchorage is required. The benefit of having additional alveolar screws is that there is no risk of contact with the roots when the teeth are moving. 15
Lower molar intrusion occurs when force is applied in a distal direction using screws positioned in the buccal shelf region. 11 Because the distalization force from the buccal shelf miniscrews crosses the mandibular dental arch's center of resistance, it causes the mandibular arch to rotate counterclockwise. 9
Considering the effects of camouflage treatment on the extraoral profile, the prominence of the chin cannot be corrected with this treatment option. Cases who'll admit camouflage treatment should be informed in advance that there will be limitations in profile change.
The buccal shelf miniscrew- supported mandibular arch distalization treatment applied in Class III malocclusion cases offers a successful preference because it eliminates the side effects seen in other camouflage treatment options.
Summary and Conclusion
The Buccal shelf implants can withstand heavier loads and
appear as a viable option for lower full arch distalisation.
When compared to retromolar implants there is no waiting
period required for bone ll in the third molar region, thus
advantage
The purpose of this report to describe technique for lower arch distalization with buccal shelf screws. These screws are made of stainless-steel and diameter is of 2mm and length 12mm placed in buccal shelf area.
We achieved full arch distalization in span of 4-5 months into Class I molar and Class I canine relationship, with normal overjet and overbite.
Source of Funding
Author received no financial support for the research, authorship, and/or publication of this article.