Introduction
The principal goal of orthodontic treatment is to provide effective and most efficient tooth movement, and this search for efficient orthodontic tooth movement has stirred the evolution of innumerable materials intended to optimize patient comfort and reduce treatment time. Friction being an imperative element in clinical orthodontics affects all stages of treatment, and high frictional forces can affect the treatment results along with duration in a deleterious manner.1
Friction, both static and kinetic friction, results from the interplay between an arch-wire, bracket, and ligature. It is well known that ligatures significantly exert friction by pressing the wire against the bracket. 2 To reduce friction on ligation, various methods and materials have been tried, like slackened steel ligatures, modified elastomeric modules, ligatures coated with fluorine-containing resins, etc. 3
Two more types of elastomeric ligatures, namely Slide ligatures (Leone, Sesto Fiorentino), and super Slick ligatures (TP Orthodontics, LaPorte, Ind) have been introduced to reduce friction at bracket-archwire interface. 4 Few clinical studies and in-vitro studies have divulged the fact that non-conventional ligatures can reduce frictional resistance equated with conventional during the initial leveling and alignment phase of orthodontic treatment. 5, 6, 7, 8= It is to be noted that maximum friction is encountered only during the retraction stage. 9 This study was done to appraise the frictional resistance of non-conventional elastomeric modules in comparison with conventional elastomeric modules during the retraction of teeth.
Top of Form
Materials and Methods
The study was commenced after obtaining ethical clearance (Ref. No.0420/DE/2016).
The sample size was estimated using G Power version 3.1.9.4, showing a sample size of 30 with a power of the statistical test set at 80% and a permissible (α) error of 5% based on the study by Dholakia K. et al. 10 The study sample includes 30 patients (11 males and 19 females) undergoing orthodontic treatment, satisfying the following inclusion criteria. The inclusion criteria are
Individuals with good physical and mental health who are not under any routine medication
Age group: 14 – 24 years
Class I molar relationship (± 1mm and overjet not exceeding 5mm
Bidental protrusion requiring extraction of all first Premolars
Well aligned maxillary and mandibular incisors
All teeth anatomically normal, vital and no congenitally missing teeth
No Previous history of orthodontic treatment and no oral habits
The study sample was grouped into 3 groups. Group A (15 study sample selected randomly) received Slide nonconventional elastomeric ligatures (Leone, Sesto Fiorentino) on canine brackets on one side and conventional ligature mode on the other side (3M modules).
Group B (15 patients selected randomly) received super slick nonconventional elastomeric ligatures (TP Orthodontics, laporte, Ind.) on canine brackets on one side and conventional ligature mode on the other side (3M modules).
Group C was the control group which received the conventional elastomeric ligature 3M (Monrovia,CA USA).
Therapeutic Extraction of all first premolars was performed. 0.022’MBT brackets were bonded. Levelling and alignment stage of orthodontic treatement were done for both arches. Once complete alignment and levelling of the arches were achieved, upper and lower arch study models were made and the distances between the canine tip and central pit of the first molar were measured with the digital vernier calliper and were considered as the baseline value. The canines were secured to the archwires with nonconventional ligature - Slide Slide ligatures and Super Slick ligatures in group A and B respectively. All other teeth except canines in both group A and group B were secured with conventional ligatures to the archwire. 150grams of retraction force was applied using the closed coil springs. The patients were recalled at 1month interval during the retraction phase of treatment. At each recall visit the arch wire were removed and checked for any damage and replaced if any damage was noted. Clinical photographs and impressions for study models were taken at each appointment. Retraction force was rechecked to be maintained at 150gms. The modules were replaced with another set in the respective quadrants.
Study model were done at: T0- (base line) – before retraction of canines; T1 – T5: At the interval of one month for approximately 5months.
The study models thus obtained were assessed for canine retraction rate and anchor loss, to quantify the canine rotation and rotation of Molar based on the method followed by Shpack et al . 11 An oval acrylic button with wire jigs was made for each maxillary and mandibular arch. The acrylic button was made in the palatal rugae region, in the maxillary arch, as the rugal area does not change with orthodontic treatment. In the mandibular arch, an oval acrylic button was made on the lingual side and a midline pointer was fabricated with the wire extending from an acrylic plug lying over the lingual alveolar region onto a point bisecting the incisor segment. Four wires made of dimension 21x22 SS were embedded in the acrylic button. The outer ends of the anterior wires, called “Anterior Wire Tip”(AWT) made to touch the canine tips while the posterior wire, called “Posterior Wire Tip”(PWT), whose outer ends measured about 10 mm and was made to coincide with central fossa of first molar(Figure 1 a, & b). The acrylic plug was made with the model obtained at T0, the plug thus prepared is fitted to the successive models taken at T1 to T5. The perpendicular distance from the tip of the canine to the PWT of the same side was measured using a digital vernier caliper and was considered to be the amount of distal movement of the canine.
Anchorage loss is measured from the models obtained. To measure the movement of each molar, the perpendicular distance from the central fossa of the molars to AWT of the same side was measured using a digital vernier caliper.
The rotation of upper canines was calculated by the angle(x) between the midpalatine suture (maxilla) or midline pointer (mandible) and a line joining the mesial and distal edges of the Canines. Total rotation is the difference between the T0 and T5 values. (Figure 2 a).
The rotation of upper canines was calculated by the angle(y) between a perpendicular line drawn posteriorly from the incisive papilla on the mid-palatine raphe in the maxilla (midline pointer in the mandible) and tangents from the distal margins of the first molars ( Figure 2 b). The differences in T0 and T5 angles quantify molar rotation. All measurements were made to the nearest 0.5 with a dome template.
Statistical analysis
One way ANOVA test was used to compare differences between 3 groups included in the study. Student t-test was done to find the significance of study parameters within two groups. A post hoc test was used for pairwise comparison of data. Test of homogeneity helped to determine the appropriate post hoc test. Tukey HSD is a type of post hoc test used in this study. [* Moderately significant (0.01<P<0.05) ** Strongly significant (P value < 0.01)]
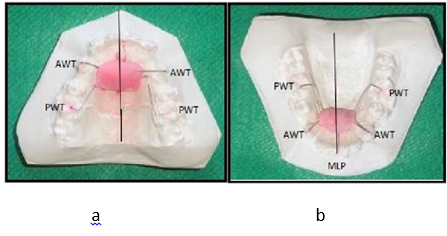
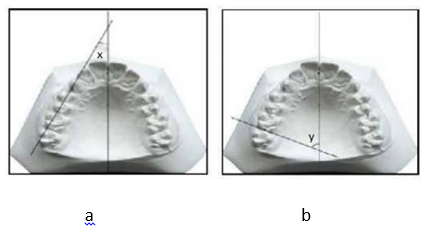
Figure 3
a; Mean Canine Retraction between groups –Maxilla b; Mean Canine Retraction between groups- Mandible
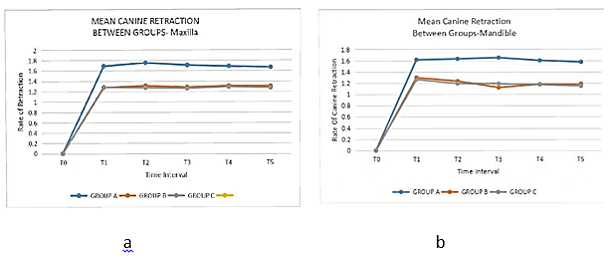
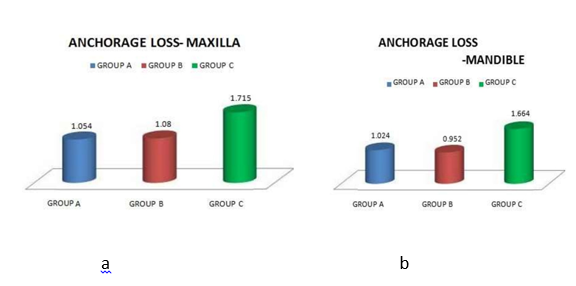
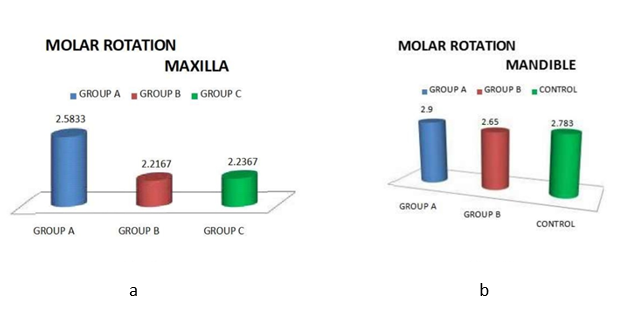
Table 1
Mean measurements in Group A-students t test
Table 2
Mean measurements in Group B-students t test
Table 3
Mean measurements in Group C-Students t test
Table 4
Mean measurements in maxilla –one way ANOVA
Table 5
Mean measurements in mandible- one way ANOVA
Result
Rate of canine retraction: In maxilla, the mean canine retraction rate for Group A, group B, and group C was 1.674+/-0.092, 1.187+/-0.156, and 1.147+/-0.113respectively (Figure 3 a). In mandible the mean canine retraction rate for Group A, group B, and group C was 1.765+0.099, 1.300+0.099 and 1.270+0.111 respectively (Figure 3 b)(Table 1, Table 2, Table 3). The difference in the retraction rate was statistically significant, ie. p<0.0001.
Anchorage loss: In maxilla group A had a mean loss of anchorage of about 1.054mm with a standard deviation of +0.174 while group B had a mean loss of anchorage of about 1.080mm with a standard deviation of +0.188. Group C had a mean loss of anchorage of about 1.715mm +0.163(Figure 4 a).
In mandible, the mean loss of anchorage was around 1.024mm, 0.952mm and 1.664mm with a standard deviation of +0.113, +0.083 and +0.111 in Group A, B and C respectively (Figure 4 b). The difference in the mesial movement of the maxillary molar was statistically significant p<0.0001.
Canine Rotation: Group A had a mean canine rotation of 8.550+1.506 in maxilla and 8.930+1.474 in mandible. Mean canine rotation for group B was 5.300+1.386 in maxilla and 5.830+1.096 in mandible. Group C had a mean canine rotation of 6.100+1.315 in maxilla and 6.880+1.813 in mandible (Figure 5 a, b).
Molar Rotation: Mean molar rotation rate in maxilla was 2.580+0.735, 2.210+0.549 and 2.210+0.700 for group A, group B and group C respectively while Mean molar rotation rate in mandible was 2.900+0.541, 2.650+0.639and 2.780+0.604 in group A, group B and group C respectively(Figure 5 a, b)(Table 4, Table 5).
Discussion
Great attention has been given to the factors influencing resistance to sliding in orthodontics, as reduced resistance to sliding leads to increased efficiency of treatment. The mode of ligation influences friction at the bracket, wire, and modules, which may extend the overall treatment time. Frictional resistance at the binding unit caused by ligation has received limited attention in the literature. It has been proved in previous studies that elastic ligatures significantly contribute to friction compared to stainless steel ligatures and exert 50gms to 150gms of force at the time of seating. 12 Slide ligatures (Leone, Sesto Fiorentino), introduced in 2005, are novel ligatures made of a special polyurethane mix contrived by the injection molding technique with the quoted advantage of the potentially reducing treatment time by reducing friction.13 The Super Slick Ties is a new polymeric-coated ligature tie (La Porte, Ind) that claims the modules become extremely slippery when wet or moistened within the oral cavity and thus reduce friction by 70%. 14 The current study was done to compare the efficacy of these Slide ligatures and Superslick ligatures over that of the conventional modules.
There have been numerous in-vitro studies done using Slide and Superslick ligatures to assess their effect on frictional characteristics. Max Hain 15 studied the effectiveness of the new slick elastomeric modules from TP Orthodontics (La Porte, Ind) and concluded that saliva-lubricated slick modules can reduce static friction at the ligature/archwire(0.019x0.025 SS) interface up to 60%. Deepu Leander 16 compared the frictional characteristics of the coated modules Super Slick Ties(SST), with those of uncoated modules(Dispense-A-Stix) in four different archwires and concluded that SST produced lower levels of friction (11%) for all archwire materials when compared to conventional uncoated modules. In 2008, Tiziano Bacetti and Lorenzo Franchi et.al 17 showed that the combination of slide ligature modules with super elastic NITI wires produced a significantly lesser amount of binding at the bracket/archwire/ligature interfaces in comparison to conventional modules during the leveling and aligning stage. The duration of orthodontic treatment is reduced during initial leveling and alignment and expansion of dental arch evident as the biomechanical consequences of the use of low friction slide ligatures. 18, 19 The current study helps to clinically gauge the efficacy of these Slide ligatures and Superslick ligatures on the rate of retraction, anchorage loss, canine, and molar rotations during the retraction stage of orthodontic treatment compared with that of the conventional methods by direct cast measurements to avoid any error resulting from magnification from the photocopies of study models, advocated by Gulati et al. 20, Ravi K et al 21
Dholakia K et al. 10 conducted a study to compare the clinical competency of conventional elastomeric ligatures and non-conventional during the canine retraction stage of treatment. The authors concluded that canine retraction rate is greater using slide ligatures but there is no significant clinical advantage observed with non-conventional ligatures over conventional concerning time required for the complete retraction and prevention of canine tipping or rotations. In the present study, the rate of canine retraction is greater using slide ligatures and the time taken for retraction using slide ligature was also much less when compared to the conventional.
In the present study, the mean canine retraction rate was 1.67mm(maxillary arch) and 1.76mm(mandibular arch) for slide ligatures and 1.18mm (maxillary arch) 1.30mm(mandibular arch) for super slick ligature which was comparable to the study conducted by Ravi K et al 21 where the mean rate of retraction on Slide ligature module side was 1.49 mm per month and that on the side of the conventional module was 1.14 mm per month. They concluded that Slide ligatures can be a suitable alternative to conventional modules because of their low friction property, which allows for a faster rate of canine retraction.
In the study by Ravi K et al 21 mean anchorage loss for the study group was1.75±0.45mm, which was comparable to the anchor loss in the control group in the current study, which was 1.71mm.
Melih Y Sueri and Tamer Turk 22 evaluated the amount of canine rotation while using Niti closed coil spring after applying 150gms and reported a mean of 7.750distopalatal rotation. This was similar to the results of the Slide ligature group. The increased rotation of canine which occurred in the slide ligature group can be ascribed to the basic structure of the Slide ligature modules, because compared to the conventional modules, slide ligature has increased bulk while super slick ligature has less rotation as it is much lighter than the conventional modules. Molar rotations were not significant in both conventional and non-conventional modes.
Hence, in the age of low friction systems, even though slide ligature modules offer a promising solution to provide ligature with reduced friction during orthodontic treatment with better control of tooth position compared to conventional modules, further refinements are desirable and further evidence based studies are essential to definitively evaluate the clinical differences between non-conventional and conventional modules on orthodontic treatment.
Conclusion
According to the results of the present study it is concluded that
The canine retraction rate was greater with Slide ligature than with conventional and super slick ligature .
Mean loss of anchorage was minimum with non-conventional modules when compared to the non conventional ligatures.
Mean canine rotation during retraction was minimal in super slick ligature and was greater in Slide ligature, which was considered to be the only disadvantage of Slide ligature.
Molar rotations were perceptible for all the study groups but is not statistically evident