Introduction
Orthodontic treatment has been widely accepted by the people of all the age groups and the main reason behind it is esthetics. The rapid pace of life and increased demand of shorter time duration for the orthodontic treatment by the patient has insisted the orthodontists to introduce various techniques which can decrease the time span of 20-24 months which is usually required for the extraction orthodontic treatment with fixed appliances. So, this leads to the introduction of diverse methods that briskly completes the orthodontic treatment.
Various attempts have been made in this direction and documented in literature to reduce the orthodontic treatment time and each approach claimed to be superior then other in different studies. 1 These attempts can be grouped mainly into three categories i.e. 1) local or systemic administration of medicines; 2) mechanical or physical stimulation which include the use of pulsed and static magnetic fields; 3) surgical methods that include alveolar surgery to undermine interseptal bone, corticotomies, dentoalveolar distraction and corticision.
All these methods induce a regional acceleratory phenomenon (RAP) (Frost 1983) which is defined as tissue reaction to a noxious stimuli that stimulates the hard tissues (bone and cartilage) as well as the soft tissues and causes increased osteoclastogenesis. 2 Basically, RAP boosts up the activation of bone multicellular units (BMU’s) which thereby escalates the remodeling in that specific area. The rapidity of the orthodontic tooth movement is influenced by bone turnover, bone density and hylanization of the PDL. 3 Numerous published studies had stated that all the above mentioned methods have the ability to influence the RAP phenomenon.
Innumerable methods have been introduced into dentistry over a period of time which are broadly classified into invasive and non invasive methods (Figure 1).
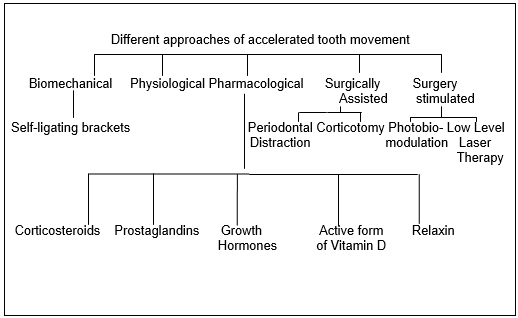
Conventional corticotomy, osteotomy are invasive methods while non invasive techniques include peizocision, peizopuncture and micro-osteoperforations and minimally invasive techniques involves cytokines, injections of prostaglandins and hormones like relaxin, thyroid and parathyroid hormones and platelet rich plasma. 2, 3, 4 All these researches were begun in 1890’s with osteotomy and later on involved several other methods mentioned above. The reason behind this ongoing research is the disadvantages associated with the invasive methods like pain, discomfort, delayed healing etc. Later on non- invasive methods were popularized which includes lasers, PRP etc. having the advantages of no pain, minimal discomfort, no delayed healing is associated with them.
Materials and Methods
The study was conducted in the Department of Orthodontics and Dentofacial Orthopedics of Genesis Institute of Dental Sciences and Research. It was a split mouth study design having 1:1 allocation in which right side was allocated as experimental side while left side was allocated as control side. Total of 40 patients were randomly selected and 10 patients were allocated in each group after statistically calculating the sample requirement. The patient selection was done on the basis of eligibility criteria and informed consent was taken after explaining the treatment procedure (Table 1).
Table 1
Inclusion & exclusion criteria
Present study investigated four different methods of accelerated orthodontic tooth movement such as micro-osteoperforations (MOP’s), corticotomies, low level laser therapy (LLLT) and platelet rich plasma (PRP).
Pre operative records were taken for the selected patients and then were bonded with MBT 0.022 X 0.028 inch brackets to the maxillary and mandibular arch. For anchorage 2nd molars were banded and molar stops were incorporated into the wire. After leveling and alignment, retraction was initiated on 0.019 X 0.025 inch stainless steel with NiTi closed coil spring and elastomeric chain delivering a force of 150 grams each side. Extraction of first premolars were done just before the initiation of canine retraction. Required blood investigations were done for patients requiring MOP’s and corticotomies. All the patients requiring invasive procedures were anaesthetized with 2% lignocaine hydrochloride (1:200000) with adrenaline while topical application of adrenaline was done for PRP therapy.
Micro-osteoperforations - The position of micro-osteoperforations was 3 mm distal to canine and 2 mm above the crest of bone. A total of 3 micro-osteoperforations of diameter 1.3 mm at a distance of 2 mm each were done with Erbium-YAG Hard Tissue Laser (frequency -20Hz, Power-8W and Energy- 400mJ). Depth of perforations was till the medullary bone. Exposure was done only once and canine retraction re-activation was done monthly (Figure 2).

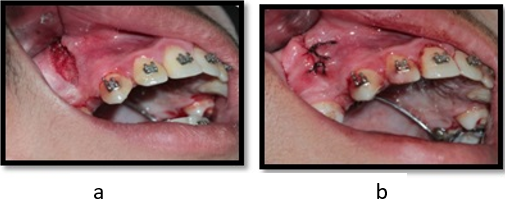
Corticision- Corticision was performed 3 mm distal to canine and 2 mm above the crest of alveolar base till 2 mm apical to root apex (fig.3a & 2b). Gingival incision was made using Erbium-YAG Hard Tissue Laser (frequency -20Hz, Power-8W and Energy- 400mJ). Depth of the cuts were till the medullary bone. Gingival tissue were then sutured back using silk sutures. Exposure was done only in the initiation of the procedure and canine retraction activation was done at an interval of 1 month.
Post operative instructions were given-
Tablet Paracetamol 500 mg was prescribed.
For first 24 hours after the operation, avoid hot beverages and food.
Avoid citrus fruits or fruit juices and highly spiced foods; as these may cause pain.
Avoid smoking.
Warm saline rinses 2-3 times daily, for one week starting 24 hours post-operatively.
Cold fermentation on the face over the operated area, for the first hour after the surgery.
Report for checkup 24 hours post-operatively, after 10 days for removal of sutures or even in between if there is any discomfort.
Low Level Laser Therapy- For LLLT soft tissue GaAlAs diode laser was used having wavelength of 800nm, power 0.25 mW, energy density of 8 J for 10 seconds (Figure 4 a & b). Each irradiation was done every 15 days for 5 months and canine retraction was activated after 1 month. irradiations were done: 5 on buccal and 5 on palatal side-:

2 irradiation doses on the cervical third of the canine root (1 mesial and 1 distal).
2 on the apical third of the canine root (1 mesial and 1 distal).
1 on the middle third.
Platelet Rich Plasma- For PRP approx. 3 ml of an autologous blood was withdrawn from which approx. 30 units of PRP was obtained. Out of which 25 units of PRP was used and injected into the 5 different sites (fig. 5a & 4b) with the help of insulin syringe i.e.- intraligamentary middle, distobuccal, distopalatal and submucosal buccal and palatal as described by Rashid et al and for each site 5 units of PRP was used.
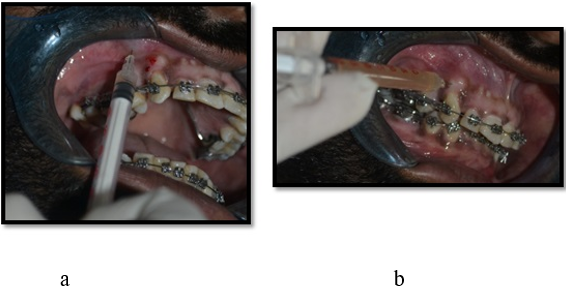
Procedure was repeated at an interval of 21 days while canine retraction re-activations was done after 6 weeks. CaCl2 was used an activating medium for the PRP. Complete records of the patient were taken monthly in MOP’s, corticision, lasers while in PRP study records were taken at an interval of 21 days. Study models were fabricated before starting canine retraction by taking alginate impressions and then models were repeated till the treatment was completed. The rate of canine retraction was measured between the two points i.e. the distal surface of canine and the mesial surface of 2ndpremolar.
For the measurement of anchor loss, the movement for the first molar was calculated using ZIelger and Ingevall (1989) method for this upper dental cast was photographed with the central projection perpendicular to the occlusal plane, together with a millimeter scale mounted in this plane. Subsequently, photographic copies were made to scale. Before taking the photograph, the median raphe was marked with a pencil on the model. The mesial contact point of the first molar was projected on the median line and the distance from this point to most prominent medial rugae was measured. This measurement was made with digital calipers. The amount of anchor loss was considered to be the difference between sequential measurements (Ex-T0-T1).
Results The measurements of the maxillary canine retraction between the different accelerating phenomenon and conventional method has been given in Table 2, Table 3, Table 4, Table 5 respectively.
omparison of the mean canine movement and mean anchor loss b/w micro- osteoperforations and conventional method from T0-subsequent time periods- (T0-T1= 1 month).
Table 2
Mean canine movement
Table 2 showed the significant results of mean canine movement and mean anchor loss b/w micro-osteoperforations and conventional method.
Right side – Experimental side; Left side- Control side.
Table 3
Comparison of the mean canine movement & mean anchor loss b/w coticision and conventional method from T0-subsequent time periods- (T0-T1= 1 month).
Table 3 showed the significant results of mean canine movement and mean anchor loss b/w corticision and conventional method.
Right side – Experimental side; Left side- Control side
Table 4
Comparison of mean canine movement & mean anchor loss b/w LLT and conventional method from T0-subsequent time periods (T0-T1= 1 month).
Table 4 showed the significant results of mean canine movement & mean anchor loss b/w LLT and conventional method.
Right side – Experimental side; Left side- Control side
Table 5
Comparison of the mean canine movement and mean anchor loss b/w PRP and conventional method (T0-T1=21 days)
Table 5 depicts the mean canine movement and mean anchor loss with PRP and conventional method.
Right side – Experimental side; Left side- Control side
The statistically analysis of the study with paired t-test revealed that there is significant difference in the tooth movement between the conventional method and different accelerating tooth movement and amongst the four different methods microosteoperforations is the best method.
Discussion
Common problems encountered by the patients during orthodontic treatment therapy are ulcerations due to irritation from distal wire component, decalcification, white spot lesions, inability to maintain oral hygiene, metallic taste, root resorption, open gingival embrasures etc. increases the total span of treatment leads to the thought of introducing acceleratory methods in orthodontics. First attempt to accelerate the orthodontic tooth movement was done in 1890’s with osteoetomy i.e. the complete bone cutting involving the cortex and medulla. 5 The major disadvantage of this method is pain, inflammation and delayed wound healing as it is an invasive method and troubles a lot which forced the orthodontists to find better ways which are less invasive as well as patient friendly. 5, 6 This thought then brought up the new method i.e corticision. Kole 1959 popularized the technique corticotomy for accelerating the tooth movement. 7 In the initial days this method was used alongwith the osteotomy but later on it was used alone. It is less invasive as compared to osteotomy but few pain and discomfort were encountered by the patient and the present study revealed that corticision is a fruitful method for accelerating the orthodontic tooth movement. 5, 6, 7 The present study shows similar results to one of the study by Patterson et al in 2016 and claims that corticomy is definitely a reliable method for pacing up the orthodontic tooth movement but as we know post operative slight discomfort can also be observed. 7 Subsequently research to found out a less invasive method was continued.
In 1998 Liou et al did pdl distraction for the acceleration of orthodontic tooth movement and there was a marked canine retraction in by 6.5 mm in 3 weeks with customized distracters but the major disadvantage of this technique was that there were increased chances of root resorption. 8 Afterwards piezocision came into existence which was popularized by Dibart et al in 2010. 9 It is less invasive than corticotomy and osteotomy but this method also involved the removal of bone and placement of grafts. But later on this method was also less accepeted by the patients because of the surgical intervention and delayed healing and less studies have been done on the effectiveness of peizocision on acceleration of orthodontic tooth movement. So, more studies are required to disclose its long term effects. 5 Then methods like resonance vibrations, static and pulsed electromagnetic fields were studied. 10 But less literature is available on the effectiveness of vibrations and electromagnetic fields on the orthodontic tooth movement. So, more studies are required for the same. Thereafter lasers came into existence. Gama et al in 2010 stated that LLLT is not an effective method but the evidences of present study reveals that LLLT can be considered as a potential method of accelerating the orthodontic tooth movement having the advantages like less invasive, painless, no fear of delayed healing etc. 11 Other effective method is micro-osteoperforations and the present study shows similar results to the study of Alikhani et al (2013) which ensures that MOP’s have the potential to accelerate the orthodontic tooth movement but slight discomfort can be seen. 12 In late 1960’s pharmacological methods were popularized like injections of parathyroid and thyroid hormone, relaxin, prostaglandins. But literature revealed that these methods are least used and study of McGorray (2011) revealed that relaxin does not affect much the orthodontic tooth movement while the prostaglandins have the ability to speed up the orthodontic tooth movement. 13 Recently, platelet rich plasma has been popularized in various streams and in orthodontics it was firstly used by Rashid et al in 2017. 14 He used mongrel dogs in which 25 units of PRP was used and his study claimed that PRP has the ability to quicken the orthodontic tooth movement. Then in 2020 Ahmed et al did a human study in which 10 healthy female patients were injected with 25 units of PRP at five different sites and revealed that PRP is a less invasive and effective technique for hasten the orthodontic tooth movement. 1 The present study shows similar results to this study which stated that PRP has the beneficial effects on the rate of orthodontic tooth movement with no or less pain, discomfort etc.
While study by Sufarnap et al (2018) is in contrast to both the studies of PRP. He stated that PRP has no effect on orthodontic tooth movement but evidences of present study denies the results of this study. 15
Conclusion
The present study reveals that all the four different methods have the ability to accelerate the orthodontic tooth movement and out of all the above methods microosteo perforations are most effective when compared with other methods. The order of effectiveness is MOPs> Corticotomy> LLT> PRP. Low Level Laser Therapy and Platelet Rich Plasma are the less invasive techniques and has least chances or no chance of pain sensation while micro-osteoperforations and corticotomies are the invasive methods. But various studies including systemic review and meta analysis needs to be done to evaluate the most effective method of tooth movement.
Summary
The need of the hour is to reduce the orthodontic treatment duration as per patient’s demand. So, various attempts have been made in this direction and numerous methods have been introduced into the dentistry which includes osteotomy, corticision, peizocicion, electromagnetic fileds, lasers, micro-osteoperforations, injections of thyroid and parathyroid hormones, relaxin, prostaglandins, platelet rich plasma etc. Countless published studies states that all different methods have the ability to accelerate the orthodontic tooth movement but which method to select will depend upon patient’s compliance as well as the advantages and disadvantages of the particular method.