Introduction
Factors such as age, sex, and ethnic group are important in making a proper orthodontic treatment plan; another important factor is the facial growth pattern and its several clinical characteristics.1 The expression of disharmonious proportions in the facial skeleton can be attributed to the failure of normal, coordinated growth of the various regions of the craniofacial complex in terms of timing, magnitude, and direction. The facial growth pattern is established at an early age, before the eruption of the maxillary first molar.2
Facial skeletal characteristics of subjects with high-angle cases include increased total face height, high mandibular plane angle, increased palatal plane angle, clockwise mandibular rotation, short mandibular ramus, and high-gonial angle. Opposite aspects are present in subjects with a low-angle case.3, 4, 5, 6, 7, 8, 9, 10 The soft tissues attempt to compensate for extremes in vertical skeletal support in those persons with long and short vertical facial patterns. Those with short facial patterns have a thinner soft tissue drape that may attempt to mask the strong appearance of the mandible in profile. Conversely, those with long vertical patterns have a thicker integumental profile, which may compensate for the lack of skeletal support. 11, 12, 13
Maxillary dental arches of low-angle cases are broader and also show increased overbite. Maxillary dental arches of high-angle cases are narrower, with posterior crossbite tendency and anterior open bite.14, 15
Andrews suggested the six keys to normal occlusion. The third key relates to crown inclination, which refers to the labiolingual or buccolingual inclination of the long axis of the crown, not to the long axis of the entire tooth. He reported a lingual inclination present in the maxillary and mandibular posterior crowns. It has been reported that the buccolingual inclination of molar crowns changes with the growth of an individual.
The present study investigated the characteristics of subjects with different facial patterns. We compared the buccolingual inclinations of the posterior teeth (1st molars) in subjects with a low-angle case (proportionally short lower anterior face height) with those in subjects with a high-angle case (proportionally long lower anterior face height) using the conventional technique (model casts).
Figure 1
Landmarks: nasion (N), anterior nasal spine (ANS), and menton (Me). Linear distances: upper anteior face height (UAFH) and lower anterior face height (LAFH). Angular measurement: mandibular plane angle (Go-Gn-SN).
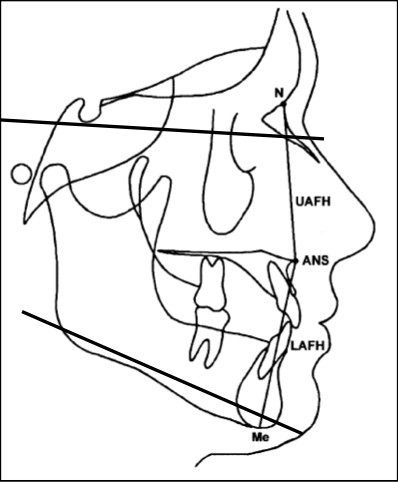
Figure 2
Trimming of base of models, parallel to posterior occlusal plane (POP), according to method described by Ross et al.

Figure 3
Occlusal view of maxillary dental study model. P, Maxillary midline; A, occlusal cut line for maxillary right molar; B, occlusal cut line for maxillary left molar; C, occlusal cut line for maxillary right premolar; D, occlusal cut line for maxillary left premolar.
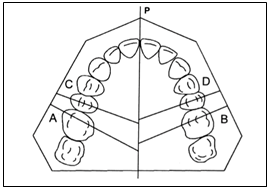
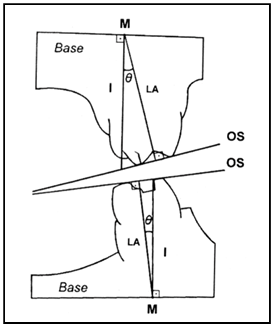
Figure 4
Anteroposterior view of both models. M, Inter- section of tooth long axis and dental study model base; LA, tooth long axis; I, line perpendicular to base of models. The angle represents relationship between tooth inclination and line perpendicular to base of model. Reproduced, withmodifications, from Ross et al.
Materials and Methods
Subjects were selected from the outpatient department of the Department of Orthodontics and Dentofacial Orthopaedics at Jaipur Dental College, Jaipur, Rajasthan. These subjects came to the department voluntarily for orthodontic treatment. Patients who had not undergone orthodontic treatment earlier. The exclusion criteria include patients having severe premolar and molar rotations, partially erupted molars, anterior open bite, any skeletal deformity, any syndrome, scissor bite and crossbite in the premolar-molar region.
20 subjects with permanent dentition were divided into 2 groups. Group I comprises 10 subjects with low-angle cases (proportionally short lower anterior facial height) and group II with high-angle cases (proportionally long lower anterior facial height). The buccolingual inclination of 1st molar was assessed on model casts.
All subjects were evaluated clinically and facial and lateral photographs were taken. The lateral cephalometric radiograph was used. The cephalograms were traced on an acetate sheet. The ratio between upper and lower anterior face height was determined to check whether either subject is low-angle or high-angle. Go-Gn-SN angle is also checked.
The following landmarks are marked on traced cephalometric sheet (Figure
Menton (Me) : the lowest point of the mandibular symphysis
Anterior nasal spine (ANS : the tip of the anterior nasal spine
Nasion(N):the anterior end of the naso-frontal suture
Gonion (Go): A point on the curvature of the angle of the mandible located by bisecting the angle formed by lines tangent to the posterior ramps and the inferior border of the mandible.
Gnathion (Gn): A point located by taking the midpoint between the anterior (pogonion) and inferior (menton) points of the bony chin.
Sella (Se): The geometric centre of the pituitary fossa
Upper anterior face height (UAFH): the distance between N and ANS (N-ANS).
Lower anterior face height (LAFH): the distance between ANS and Me (ANS-Me).
The mandibular angle is also measured from (Go-Gn-SN). If the angle is less than 32°are considered low-angle cases (horizontal growth pattern) and if the angle is more than 32° are considered high-angle cases (vertical growth pattern).
The 20 dental study models (maxillary and mandibular pretreatment dental study models from the 20 subjects) were taken. The POP was formed by the three most occlusally located cusps of the two first molars and one or both of the premolars The base of the models was trimmed parallel to the POP. The angle formed by the molar occlusal surface and the POP was determined by trimming the heel of each cast perpendicular to its base (and POP) and parallel to the occlusal line that connects the mesiobuccal and mesiolingual cusp tips through the buccal groove. The right and left heels of each cast were photocopied independently. The inclination of the occlusal surface (OS) was reported as the angle formed by a perpendicular to the OS line and its intersection with the model base, plus or minus 90°. The angle was termed positive when the molar was buccally inclined and negative when the molar was lingually inclined.16
Andrews tried to determine the tooth crown inclination, considering the facial axis of the clinical crown and the occlusal plane that passes through the anterior and posterior teeth. The orthodontic study models were sequentially divided into right and left halves through the P cut (Figure 3). The distal portions of each side were then trimmed perpendicularly to their base (and to the POP) up to the occlusal lines (A and B cuts) that pass through the mesiobuccal and mesiolingual cusps of the first molars (Figure 3). The mesial portions of each side were also trimmed perpendicularly to their base and up to the occlusal lines (C and D cuts) that pass through the buccal and lingual cusps (mesiolingual cusp for the mandibular teeth) of the second premolars (Figure 3).
Independent photocopies of the study models were obtained for each quadrant, from the cuts of the first molar and second premolar from both the right and left sides, to determine the planes and angles of interest. Photocopies from partially erupted teeth or teeth with significant rotation were rejected. The M point was obtained by the intersection of the tooth long axis and the dental study model base, from which a line perpendicular to the base was drawn (I line)(Figure 4). Therefore, the angle was obtained between this line and the tooth long axis; it indicated the buccolingual inclination of the occlusal surface of the first molars and second premolars. The angle was positive when the long axes of these teeth (as obtained from the occlusal surfaces) had a buccal inclination, and negative in cases of lingual inclination.
Result
Mean Value= GROUP I (horizontal growth pattern) shows 1.1° and in GROUP II (vertical growth pattern) shows 5°. Median value calculated for group I (horizontal growth pattern) is 1 and in group II (vertical growth pattern)
Discussion
The skeletal differences that lead to disproportionate lower face height in long-faced and short-faced children are related to mandibular morphology. The length of the body and ramus of the mandible is similar to that of normal children, but the gonial angle is greatly increased or decreased, respectively. 17 There was an inverse correlation between the upper and the lower anterior and posterior dentoalveolar heights and the ratio UAFH/LAFH, that is, as the ratio increases, the dentoalveolar height decreases. In cases with decreased UAFH/LAFH ratio value (long LAFH), the dentoalveolar height will usually be increased as well, consequently extruding forces on the dentition should be avoided. Evaluation of environmental influences, such as airway obstruction, should also be performed because there is evidence that a severely obstructed airway is in some instances related to increased or increasing LAFH.On the other hand, cases with short lower anterior face height (large UAFH / LAFH ratio value) or with decreasing lower face height usually present a clear airway passage. In these cases, the dentoalveolar height is also decreased and extrusive forces can and sometimes have to be used to improve the vertical relationships.18
Table 1
Showsthe buccolingual inclination of maxillary 1st molar in Group I (horizontal) andGroup II (vertical growth pattern)
|
Sample no. |
Group I |
Group II |
|
1 |
0° |
4° |
|
2 |
1° |
6° |
|
3 |
1° |
5° |
|
4 |
2° |
4° |
|
5 |
2° |
6° |
|
6 |
0° |
5° |
|
7 |
1° |
4° |
|
8 |
2° |
4° |
|
9 |
0° |
7° |
|
10 |
2° |
5° |
The buccolingual inclination angle does not correspond to the actual long-axis inclination of the teeth but, rather, to the occlusal surface inclination, as evaluated by connecting a line between the mesiobuccal and mesiolingual cusp tips of the posterior teeth.
When there is a severe discrepancy between dental and skeletal, extraction of permanent teeth is usually indicated. However, slight-to-moderate discrepancies between dental and skeletal can be corrected by reducing dental structures by interproximal stripping, expanding the dental arch, or a combination of both. Therefore, when slight or moderate crowding is associated with a narrow dental arch and not with increased dental size, procedures to increase arch dimensions might be considered, to avoid the need for extractions. 19, 20, 21, 22, 23
The suggestion of Howe et al.,24, 25, 26, 27, 28, 29 to treat borderline patients with palatal expansion and buccal inclination of the mandibular posterior teeth, is especially applicable for those with horizontal facial patterns, as compared with those with vertical growth patterns. A common collateral effect of maxillary expansion is buccal tipping of the maxillary posterior teeth.30, 31, 32, 33 Therefore, because of the greater palatal inclination of the maxillary posterior teeth in this facial pattern, a greater maxillary expansion could be carried out without causing an accentuated and unfavourable buccal tipping of the posterior teeth, which could lead to a greater relapse of the expansion.