- Visibility 42 Views
- Downloads 5 Downloads
- DOI 10.18231/j.jco.2024.072
-
CrossMark

A comparison of treatment effects produced by AdvanSync and forsus fatigue resistant device in growing class II patients - An study
- Author Details:
-
 Saumya Upadhyay *
Saumya Upadhyay *
-
Jyothikiran Hurkadle
-
Suma Shankarappa
-
Raghunath N Rao
-
Madhuvanthi Gopalakrishnan
Introduction
Angle first described Class II malocclusion in the 1890s. It is second most common malocclusion after class I.[1] The prevalence of Class II malocclusion was reported 19.56% globally[2] and 14.6% in India.[3]
The class II malocclusion problem can be attributed to either retrognathic mandible or prognathic maxilla or a combination of both. Retrusion of mandible was found to be the most common etiological factor in this malocclusion.[4]
Management of class II malocclusion becomes intricate because of its variable etiology[5] and the age at which the patient presents to the orthodontists. During 1900s first fixed functional appliances (FFA) emerged and then plethora of appliances followed. If timed correctly, FFA can be an asset in patients with lesser growth potential[6] and also helps in avoiding any future invasive surgical interventions during adulthood.[7] he latest appliances are designed to decrease the treatment duration and reduce the need for patient co-operation[8] while allowing complete utilisation of growth left.
Amongst various appliances AdvanSync™2 molar to molar appliance appears to be the latest addition to FFA in orthodontist’s arsenal for treating class II malocclusion with mandibular retrusion whereas Forsus™ Fatigue Resistance Device (FFRD) is the most widely accepted and used FFA.
FFRD has some disadvantages like it can only be installed after pre functional levelling and alignment is achieved till 19X25 SS wire, frequent dislodgement, causes lower incisor proclination, and requires extensive anchorage preparation.
AdvanSync™2 and MARA appliances allows concurrent full fixed treatment as there is no need to level and align both arches before installation which is beneficial in terms of growth considerations as well as duration of the treatment. AdvanSync™2 has shorter arms and is engaged from molar to molar which reduces direct force transfer on mandibular canine thereby reducing lower incisor proclination effect
Therefore, understanding the appliance design, treatment processes, and comparison of the treatment effects of various FFA will enable better treatment planning and help in obtaining optimal results.
The aim of this study was to compare the differences in the skeletal, dentoalveolar and soft tissue changes produced by the AdvanSync™2 and the Forsus™ Fatigue Resistance Device fixed functional appliances in growing patients, to correct class II division I malocclusion, due to retrognathic mandible.
Materials and Methods
Method of collection of data and ethical clearance
The sample comprised of patients who reported to the Department as outpatients. Patient selection was done based on inclusion and exclusion criterias of the study. The sample size was taken as 10 per group, Group 1 (AdvanSync™2) and Group 2 (Forsus™ Fatigue Resistance Device). The investigation was approved by the Institutional Ethics Committee after critically reviewing the research protocol and registration number 59/2020 was assigned to this study.
Sample size calculation
We sought a desired level of significance (α) of 0.05, which corresponds to a 95% confidence level, to determine the necessary sample size for this paper. The required power (β), which equals 80% power, was set at 0.20. For the population under study, an estimated standard deviation (σ) of 4.70 was considered.
The following equation is used to determine the necessary sample size (n):
n = (Zα + Zβ) ² × σ² / d²
This computation yielded an approximate sample size (n) of 19. The sample size, however, was rounded up to the nearest whole number because it had to be a whole number, yielding a sample size of 20.
|
Inclusion criteria |
Exclusion criteria |
|
1. Adolescent males and females patients having class II div I malocclusion due to mandibular retrusion |
1. Class II patients with vertical growth pattern |
|
Withdrawal criteria: 1. Patient who discontinues from the study during the research. 2. Patient who has migrated from the area. |
Methodology
In Group 1 patients
Alginate impressions were taken, and the appropriate size of AdvanSync™2 (ORMCO) molar band was chosen and cemented. A telescopic rod was connected to housing on U6 and L6 molar bands, based on the desired activation. Midline correction was achieved by adding c spacers during monthly appointments. The appliance was installed without leveling and aligning, along with bonding from the second premolar to second premolar. Lower anteriors utilized Damon low torque brackets to prevent proclination. It was advised to use figure-eight-lacing from molar to molar.
Wire adjustments were made during subsequent appointments, gradually activating the appliance until achieving a overcorrected class 1 canine and molar relation
Group 2 patients
Subjects were fully banded and bonded to achieve levelling and alignment till 19X25 SS wire was placed in both the arches and cinched. Labial root torque was incorporated in the wires.
Measurements were taken using the gauge provided with the appliance and suitable length was chosen for Forsus™ Fatigue Resistance Device fatigue resistant device (3M unitek ). The EZ module was inserted into the molar buccal tube from mesial side unitil it clicks into the place. (Suppl [Figure 5]). Split crimps were used for activation of appliance during the subsequent appointments until overcorrected class 1 canine and molar relation was achieved
In both the groups, appliances were removed and fixed orthodontic treatment was continued to achieve adequate occlusion and finish.
Radiographic method
Lateral cephalograms and photographs were taken as part of the routine diagnostic records. They were taken at two times, pre treatment (T1) and post functional orthodontic treatment (T2). The measurements were done by three operators and average was taken. A total of 9 angular,12 linear measurements and 10 soft tissue variables were considered in cephalometric analysis. (Suppl [Figure 6])





|
|
Variables |
AdvanSync™2 appliance Mean difference |
Forsus™ Fatigue Resistance Device appliance - Mean difference |
P value |
|
Angular |
SNA |
1.150 |
0.900 |
0.028* |
|
SNB |
-0.900 |
-2.200 |
0.198 |
|
|
ANB |
2.050 |
2.600 |
0.712 |
|
|
MPA |
-1.300 |
1.100 |
0.168 |
|
|
L1MPA |
-2.100 |
7.100 |
0.097 |
|
|
FHPP |
-0.900 |
1.300 |
0.402 |
|
|
U1FH |
10.300 |
6.700 |
0.002* |
|
|
Gonial |
-1.800 |
-1.400 |
0.047 |
|
|
SOFT TISSUE |
Facial Angle |
-0.600 |
-2.600 |
0.248 |
|
Facial Convexity157.6 |
-1.000 |
-3.600 |
0.404 |
|
|
H Angle |
1.900 |
2.300 |
0.02* |
|
|
Nasolabial Angle |
-8.900 |
-13.700 |
0.401 |
|
|
Mentolabial Sulcus |
1.900 |
2.000 |
0.821 |
|
|
Subnasale To H Plane |
1.500 |
2.200 |
0.001* |
|
|
Upperlip E Line |
0.700 |
1.000 |
0.027 |
|
|
Lower Lip E Line |
-1.100 |
0.000 |
0.015* |
|
|
Upper Lip To Ptv |
1.300 |
0.000 |
0.015* |
|
|
Lower Lip To Ptv |
-2.000 |
-2.000 |
0.411 |
|
|
LINEAR |
Overjet |
4.950 |
3.300 |
0.014* |
|
Overbite |
1.400 |
1.600 |
0.6 |
|
|
COGN |
-3.800 |
-2.900 |
0.565 |
|
|
U1VRP |
0.900 |
1.100 |
0.921 |
|
|
L1VRP |
-0.300 |
-0.700 |
0.759 |
|
|
U6VRP |
2.200 |
-0.200 |
0.534 |
|
|
L6VRP |
-1.300 |
-1.000 |
0.341 |
|
|
U1HRP |
-2.700 |
-1.300 |
0.799 |
|
|
L1HRP |
-4.800 |
-1.300 |
0.574 |
|
|
U6HRP |
-0.900 |
-5.100 |
0.206 |
|
|
L6HRP |
-3.000 |
-1.300 |
0.006* |
|
|
LAFH |
-3.000 |
-2.000 |
0.774 |
|
|
Variables |
Mean ± SD |
Mean ± SD |
Mean difference |
P VALUE |
|
Angular |
SNA |
81.10 ±3.213 |
79.95 ±3.166 |
1.150 |
.000* |
|
SNB |
74.95 ±3.166 |
75.80 ±3.048 |
-0.900 |
.000* |
|
|
ANB |
6.20±1.398 |
4.15±0.669 |
2.050 |
.015 |
|
|
MPA |
21.70±4.448 |
23.00±5.055 |
-1.300 |
.000* |
|
|
L1MPA |
108.20±7.005 |
110.30±4.809 |
-2.100 |
.000* |
|
|
FHPP |
2.50±1.900 |
3.40±2.951 |
-0.900 |
.006* |
|
|
U1FH |
119.00±14.937 |
108.70±8.744 |
10.300 |
.044* |
|
|
GONIAL |
68.20±4.849 |
70.00±4.876 |
-1.800 |
.000* |
|
|
SOFT TISSUE |
FACIAL ANGLE |
88.40±1.776 |
89.00±4.714 |
-0.600 |
1.000 |
|
FACIAL CONVEXITY157.6 |
157.60±6.222 |
158.60±5.441 |
-1.000 |
.000* |
|
|
H ANGLE |
23.40±3.534 |
21.50±3.206 |
1.900 |
.001* |
|
|
NASOLABIAL ANGLE |
93.40±9.732 |
102.30±13.233 |
-8.900 |
.004* |
|
|
MENTOLABIAL SULCUS |
8.10±1.370 |
6.20±1.619 |
1.900 |
.001* |
|
|
SUBNASALE TO H PLANE |
9.50±2.550 |
8.00±2.667 |
1.500 |
.055* |
|
|
UPPERLIP E LINE |
0.50±2.506 |
-.20±1.814 |
0.700 |
.129 |
|
|
LOWER LIP E LINE |
-0.35±3.448 |
0.75±2.252 |
-1.100 |
.011* |
|
|
UPPER LIP TO PTV |
69.50±4.478 |
68.20±4.417 |
1.300 |
.003* |
|
|
LOWER LIP TO PTV |
63.40±5.358 |
65.40±5.910 |
-2.000 |
.003* |
|
|
LINEAR |
OVERJET |
8.25±3.066 |
3.30±0.483 |
4.950 |
.260 |
|
OVERBITE |
4.20±1.033 |
2.80±0.632 |
1.400 |
.508 |
|
|
COGN |
100.60±5.854 |
104.40±5.038 |
-3.800 |
.000* |
|
|
U1VRP |
68.60±6.867 |
67.70±6.961 |
0.900 |
.009* |
|
|
L1VRP |
63.20±6.179 |
63.50±7.153 |
-0.300 |
.000* |
|
|
U6VRP |
28.80±5.308 |
26.60±6.257 |
2.200 |
.000* |
|
|
L6VRP |
25.50±5.662 |
26.80±6.546 |
-1.300 |
.001* |
|
|
U1HRP |
67.50±2.759 |
70.20±4.392 |
-2.700 |
.001* |
|
|
L1HRP |
61.30±3.302 |
66.10±5.152 |
-4.800 |
.002* |
|
|
U6HRP |
56.90±2.378 |
57.80±4.185 |
-0.900 |
.000* |
|
|
L6HRP |
62.40±2.319 |
65.40±3.502 |
-3.000 |
.000* |
|
|
LAFH |
58.60±4.088 |
61.60±3.307 |
-3.000 |
.004* |
|
|
Varuables |
Mean ± SD |
Mean ± SD |
Mean difference |
P Value |
|
Angular |
SNA |
81.10±1.792 |
80.20±1.874 |
0.900 |
.000* |
|
SNB |
75.30±1.494 |
77.50±2.461 |
-2.200 |
.031* |
|
|
ANB |
5.30±1.252 |
2.70±1.160 |
2.600 |
.116 |
|
|
MPA |
23.80±3.360 |
22.70±3.622 |
1.100 |
.000* |
|
|
L1MPA |
110.00±7.846 |
102.90±9.620 |
7.100 |
.101 |
|
|
FHPP |
2.90±4.095 |
1.60±.503 |
1.300 |
.002* |
|
|
U1FH |
120.00±5.011 |
113.30±270 |
6.700 |
.173 |
|
|
GONIAL |
69.30±3.164 |
70.70±2.359 |
-1.400 |
.000* |
|
|
Soft Tissue |
FACIAL ANGLE |
85.90±1.197 |
88.50±.850 |
-2.600 |
.445 |
|
FACIAL CONVEXITY |
155.70±3.713 |
159.30±4.322 |
-3.600 |
.005* |
|
|
H ANGLE |
24.30±1.252 |
22.00±.789 |
2.300 |
.010 |
|
|
NASOLABIAL ANGLE |
95.20±6.250 |
108.90±6.008 |
-13.700 |
.611 |
|
|
MENTOLABIAL SULCUS |
6.00±1.414 |
4.00±1.155 |
2.000 |
.013* |
|
|
SUBNASALE TO H PLANE |
10.30±.949 |
8.10±.994 |
2.200 |
.371 |
|
|
UPPERLIP E LINE |
1.10±1.595 |
.10±1.197 |
1.000 |
.507 |
|
|
LOWER LIP E LINE |
1.60±2.271 |
1.60±.699 |
0.000 |
.074 |
|
|
UPPER LIP TO PTV |
69.50±6.399 |
69.50±5.911 |
0.000 |
.002* |
|
|
LOWER LIP TO PTV |
62.90±6.557 |
64.90±5.744 |
-2.000 |
.000* |
|
|
Linear |
OVERJET |
6.30±1.767 |
3.00±1.054 |
3.300 |
.000* |
|
OVERBITE |
3.70±1.059 |
2.10±.316 |
1.600 |
.213 |
|
|
COGN |
103.80±5.959 |
106.70±6.533 |
-2.900 |
.000* |
|
|
U1VRP |
72.00±5.774 |
70.90±.460 |
1.100 |
.000* |
|
|
L1VRP |
67.70±5.498 |
68.40±6.467 |
-700 |
.000* |
|
|
U6VRP |
30.30±6.667 |
30.50±6.671 |
-.200 |
.000* |
|
|
L6VRP |
29.70±6.567 |
30.70±433 |
-1.000 |
.009* |
|
|
U1HRP |
68.00±3.333 |
69.30±4.296 |
-1.300 |
.346 |
|
|
L1HRP |
67.20±4.984 |
68.50±4.062 |
-1.300 |
.006* |
|
|
U6HRP |
56.80±9.151 |
61.90±3.784 |
-5.100 |
.901 |
|
|
L6HRP |
63.50±6.258 |
64.80±5.554 |
-1.300 |
.012* |
|
|
LAFH |
60.30±3.164 |
62.30±.093 |
-2.000 |
.000* |
Results
Data was analysed using SPSS software version 26, and checked for normality using Kolmegorov smirnov test. Data was normality distributed. Comparison of pre-operative and post-operative changes in linear, angular and soft tissue measurements among AdvanSync™2 appliance and Forsus™ Fatigue Resistance Device appliance was carried out using paired T test. Comparison of AdvanSync™2 appliance and Forsus™ Fatigue Resistance Device appliance for overall linear, angular and soft tissue measurements was done using unpaired t test. The level of significance was kept as less than 0.05.
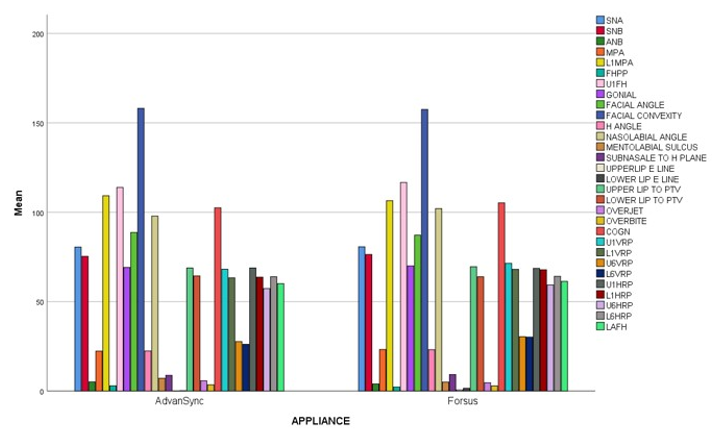
The overall Comparison of AdvanSync™2 appliance and Forsus™ Fatigue Resistance Device appliance, using unpaired T test in total study population for linear, angular and soft tissue measurements, showed significant difference among SNA angle, U1FH, H angle, subnasale to H plane, lower lip E line, upper lip to Ptm, overjet, L6HRP. ([Table 1] and [Figure 1]).
At individual level comparisons, skeletal parameters showed positive improvement in majority parameters of both the appliances. Initially the pre-operative(T1) and post-operative(T2) changes in cephalometric analysis using paired T test, among AdvanSync™2 appliance and Forsus™ Fatigue Resistance Device appliance group. ([Table 2], [Table 3])
Discussion
There are several treatment approaches being employed to address class II malocclusion. In this study, lateral cephalogram was chosen to study and compare the treatment effects of AdvanSync™2 and FFRD. It is a widely used diagnostic tool for examining skeletal, dental, and soft tissue craniofacial morphology. In this study, horizontal reference plane and vertical reference planes were derived to give standardization for correlation of pre-treatment and post functional orthodontic treatment results. [9]
The goal of adopting a functional appliance is to take advantage of remaining active growth phase and assist forward jaw posture, which cause the condylar head to develop and the glenoid fossa to remodel. [10] It has been observed that the efficiency of treatment of mandibular growth deficiencies is significantly dependent on the biological responsiveness of the condylar cartilage, which sequentially is dependent on the mandibular growth rate. [11] The resulting skeletal changes have been attributed to morphologic adaptations to altered muscular tone and a shift in masticatory muscle traction direction. A myostatic reflex is elicited, resulting in isometric contractions that stimulate the protractor muscles while inhibiting the mandibular retractor muscles. [12], [13]
Forsus™ Fatigue Resistance Device is a widely accepted FFA. It is attached from maxillary molar buccal tube to lower archwire distal to the mandibular canine which leads to direct force on incisor causing proclination. [14] The other disadvantages include cheek irritation and frequent dislodgement of rod. The cases treated with the appliance requires levelling and aligning of both the arches and should be kept in 19x25 SS prior to installation. It is amongst the drawbacks when the patient has minimal growth potential left.
AdvanSync™2 appliance is a molar to molar appliance which elimination direct force on canine and permits simultaneous orthodontic and orthopaedic corrections as it is not necessary to align and level the arches prior to its placement. Therefore, it becomes possible to capitalize on residual growth and reduce the duration of treatment. The appliance is approximately half the size of the former FFRD. It fits more conveniently in the back of the mouth due to its smaller size.
All the fixed functional appliances invariably cause lower incisor flaring. Gandedkar and Celikoglu et al. [13] study showed that it was one of the consistent drawback of all the FFA. This study also compared the effect on lower incisor inclination by both the devices. AdvanSync™2 caused comparatively less proclination than the FFRD
The appliance were inserted at a mean age of 12-14 years of age with CVMI(16) 3-5 for 6-8 months. The findings demonstrated that, at the conclusion of the functional appliance period, only minor differences, predominantly dentoalveolar, existed between two appliances.
There are several scientific literatures on the therapeutic effects of Forsus™ Fatigue Resistance Device, but relatively few [15] on the AdvanSync™2 device. There is a scarce literature comparing the treatment effects of FFRD with the AdvanSync™2 appliance. Therefore, this study was done to compare and analyze the effects of two most used appliances.
The treatment effects of both the appliances can be divided into three broad categories –
Skeletal, Dentoalveolar and Soft tissue changes on maxilla and mandible
Skeletal effects
The mandibular effects can be attributed to anterior force [14] generated from the appliances while forward positioning of the mandible and maxillary effects can be attributed to reciprocal effect of the mandibular advancement caused by the appliance. [16]
Both the appliances showed increase in SNB angle (p<0.05), suggesting mandibular advancement. There was significant increase in mandibular length in both groups. (group 1= and group 2= ). AdvanSync™2 finding were consistent with the all previous studies except study which compared treatment effects of MARA and AdvanSync™2 [17]
Both the appliances showed reduction in SNA angle but was more with AdvanSync™2 appliance. Studies Raghav P et al. [18] and Jayachandran S et al concluded that AdvanSync™2 has headgear like effect. [19] Group 2 findings were consistent with the previous published studies. [20], [21], [22])
Decrease in ANB was seen with both the appliances which suggests improvement in relative anteroposterior position between the maxilla and mandible. [8]
The mandibular plane angle, gonial angle as observed by comparison cephalometric analysis showed increase in value in Group 1 therefore must be used cautiously in patients with vertical growth pattern. [15] Group 2 had less significant effects on mandibular plane angle and gonial angle than AdvanSync™2.
There was significant increase in lower anterior facial height with AdvanSync™2 group when compared to Forsus™ Fatigue Resistance Device group and was found to be consistent with all previous studies. [12], [15], [23]
Dentoalveolar Effects
The most important drawback of Fixed Functional Appliance is lower incisor proclination. Though some of the proclination changes can be attributed to relative intrusion. [24] FFRD group showed more proclination in L1MP angle and intrusion of lower anteriors than AdvanSync™2group which was consistent with the previous studies. [15] Low torque brackets (-11°) were used in combination with AdvanSync™2 appliance which might have prevented flaring of lower anteriors.
Both the appliances showed significant changes in the U1FH angle, U1HRP and U1VRP distance which suggests retroclination , extrusion and distalisation maxillary anteriors. [8], [24], [15] The extrusion of upper incisors was more in to AdvanSync™2group.
Mesialisation and intrusion of the L6(15) was more with AdvanSync™2. It can attributed to direct reciprocal force transfer to molar since it is a molar to molar appliance
Both the appliances showed distalisation and extrusion effect on upper molars but was significant with FFRD. The dentoalveolar effects were consistent with the previous studies. [25]
Al jewair et al [24] concluded that there was no significant effect on U6, which is not in accordance with present study. The evaluation of dentoalveolar effect of Forsus™ Fatigue Resistance Device showed similar effects to the previous study [26] except U6 extrusion.
Soft Tissue Changes
In modern orthodontics, facial esthetics is one of the primary factors motivating the patient to seek orthodontic treatment. Thus, the assessment of the patient's facial soft tissue is of great importance during orthodontic diagnosis and treatment planning. Pre and post treatment values showed significant soft tissue changes by both the appliances which resulted in improved facial esthetics
Soft tissue analysis of AdvanSync™2 group revealed significant increase in linear distance of lower lip from E line and PTV suggesting protrusion and forward displacement of lower lip. There was decrease seen in upper lip to Eline and PTV distance suggesting reduction protrusion of upper lip.
Comparison of pre-treatment to post-treatment Cephalometric values suggested improvement in H angle and nasolabial angle which indicates improvement in profile. FFRD showed more significant soft tissue changes in terms of facial convexity. This was in accordance with previous study (8) but the other studies did not report any significance change. [15] Both the appliances showed increase in the facial angle but was not statistically significant. [27]
Conclusion
This study concluded that –
Both the appliance were established as reliable as they were effective in correcting Class II malocclusions with mandibular retrusion.
The AdvanSync™2 Class II corrector enabled correction of the Class II malocclusion with shortened treatment time and was more comfortable for the patient as it is smaller in size and without the rod getting dislodged frequently as inFFRD. Maxillary restriction was more significant and mandibular advancement was higher in FFRD group.
Intrusion, mesialisation of lower molars and distalisation of upper molars was seen. FFRD caused significant extrusion and distalisation of upper molars.
Both the appliances led to lower incisor proclination but it was lesser with AdvanSync™2 appliance.
Both the appliance showed retroclination and extrusion of upper incisor. It was more with AdvanSync™2 appliance.
Pre and post treatment values showed significant soft tissue changes by both the appliances which resulted in improved facial esthetics.
Scope for Future Studies
AdvanSync™2 is molar to molar appliance, thus upper and lower molar bear the forces exerted during forward positioning. Second molar bonding will be useful to minimise distalisation effects on upper molars and mesiolingual rotation and intrusion of lower molars along with figure of 8 from molar to molar.
Because of the scarce literature, further researches are needed to provide a proof of these effects which will enable us to utilise the full potential of the appliances.
Number of patients can be increased and 3D Imaging can be used in further studie
Source of Funding
None.
Conflict of Interest
None.
References
- GF Ferrazzano, T Cantile, G Sangianantoni, A Ingenito, S Rengo, B Alcidi. Oral health status and Unmet Restorative Treatment Needs (UTN) in disadvantaged migrant and not migrant children in Italy. Eur J Paediatr Dent 2019. [Google Scholar]
- MS Alhammadi, E Halboub, MS Fayed, A Labib, C El-Saaidi. Global distribution of malocclusion traits: A systematic review. Dental Press J Orthod 2018. [Google Scholar]
- P Balachandran, C Janakiram. Prevalence of malocclusion among 8-15 years old children, India - A systematic review and meta-analysis. J Oral Biol Craniofac Res 2021. [Google Scholar]
- GV Fisk, MR Culbert, RM Grainger, B Hemrend, R Moyers. The morphology and physiology of distoclusion. A summary of our present knowledge. Am J Orthod 1953. [Google Scholar]
- C Dolce, D A Mansour, S P Mcgorray, T T Wheeler. Intrarater agreement about the etiology of Class II malocclusion and treatment approach. Am J Orthod Dentofac Orthop 2012. [Google Scholar]
- S Ruf, H Pancherz. Herbst/multibracket appliance treatment of Class II division 1 malocclusions in early and late adulthood. A prospective cephalometric study of consecutively treated subjects. Eur J Orthod 2006. [Google Scholar]
- MT O’reilly, GJ Yanniello. Mandibular growth changes and maturation of cervical ertebrae. A longitudinal cephalometric study. Angle Orthod 1988. [Google Scholar]
- MH El Mofty, SA Ibrahim, OS El-Shall, WA Tawfik. Evaluation of Dentoskeletal Changes Accompanying the Treatment of Class II Malocclusion by Advansync Appliance versus Intermaxillary Coil Spring Mechanics. Al-Azhar Dent J Girls 2018. [Google Scholar]
- P Cozza, T Baccetti, L Franchi, De Toffol, L Mcnamara. Mandibular changes produced by functional appliances in Class II malocclusion: A systematic review. Am J Orthod Dentofac Orthop 2006. [Google Scholar]
- Napat Nalamliang, Udom Thongudomporn. Masticatory Muscle Responses to Mandibular Forward Positioning Appliances. J DENT ASSOC THAI 2020. [Google Scholar]
- M Celikoglu, T Unal, M Bayram, C Candirli. Treatment of a skeletal class II malocclusion using fixed functional appliance with miniplate anchorage. Eur J Dent 2014. [Google Scholar]
- BK Thushar, S Verma. Treatment outcomes in the sagittal and vertical dimensions with the AdvanSync2 class II corrector-a case series. J Contemp Orthod 2018. [Google Scholar]
- GO Cericato, M Bittencourt, LR Paranhos. Validity of the assessment method of skeletal maturation by cervical vertebrae: A systematic review and meta-analysis. . Dentomaxillofac Radiol 2015. [Google Scholar]
- S Borghei, J Broadbent, R Stevens, K Chaudhry, K Subramani. Orthodontists’ preference on type of rigid fixed functional appliance for skeletal Class II correction: A survey study. J Clin Exp Dent 2020. [Google Scholar]
- S Jayachandran, WA Wiltshire, SM Hayasaki, F Pinheiro. Comparison of AdvanSync and intermaxillary elastics in the correction of Class II malocclusions: A retrospective clinical study. Am J Orthod Dentofac Orthop 2016. [Google Scholar]
- BK Thushar, S Verma. Treatment outcomes in the sagittal and vertical dimensions with the AdvanSync2 class II corrector-a case series. J Contemp Orthod 2018. [Google Scholar]
- BK Thushar, S Verma. Treatment outcomes in the sagittal and vertical dimensions with the AdvanSync2 class II corrector-a case series. J Contemp Orthod 2018. [Google Scholar]
- M Goyal, S Madhok, S Mishra, S Kumar. evaluation of the dentoskeletal and soft tissue profile changes in skeletal class ii patients treated with advansync tm 2 fixed functional appliance -a prospective clinical trial evaluation of the dentoskeletal and soft tissue profile changes in skeletal. TMU J Dent 2019. [Google Scholar]
- CF Mir, MP Major, PW Major. Soft tissue changes with fixed functional appliances in class II division 1: A systematic review. Angle Orthod 2006. [Google Scholar]
- H Li, X Ren, Y Hu, L Tan. Effects of the forsus fatigue-resistant device on skeletal class ii malocclusion correction. J Contemp Dent Pract 2020. [Google Scholar]
- V Giuntini, A Vangelisti, C Masucci, E Defraia, JA Mcnamara, L Franchi. Treatment effects produced by the Twin-block appliance vs the Forsus Fatigue Resistant Device in growing Class II patients. Angle Orthod 2015. [Google Scholar]
- P Raghav, S Mathur, K Amit, S Mohan. Therapeutic effectiveness of advansync2 at different stages of skeletal maturity in skeletal class ii malocclusion: A single-blind clinical trial. APOS Trends Orthod 2020. [Google Scholar]
- M Goyal, S Madhok, S Mishra, S Kumar. evaluation of the dentoskeletal and soft tissue profile changes in skeletal class ii patients treated with AdvanSync™2tm 2 fixed functional appliance -a prospective clinical trial evaluation of the dentoskeletal and soft tissue profile changes in skeletal. TMU J Dent 2019. [Google Scholar]
- Al-Jewair Ts Preston, CB Moll, EM Dischinger. A comparison of the MARA and the AdvanSync functional appliances in the treatment of Class II malocclusion. Angle Orthod 2012. [Google Scholar]
- V Arora, R Sharma, S Chowdhary. Comparative evaluation of treatment effects between two fixed functional appliances for correction of Class II malocclusion: A single-center, randomized controlled trial. Angle Orthod 2018. [Google Scholar]
- G Cacciatore, L Ghislanzoni, L Alvetro, V Giuntini, L Franchi. Treatment and posttreatment effects induced by the Forsus™ Fatigue Resistance Device appliance: A controlled clinical study. Angle Orthod 2014. [Google Scholar]
- BK Thushar, S Verma. Treatment outcomes in the sagittal and vertical dimensions with the AdvanSync2 class II corrector-a case series. J Contemp Orthod 2018. [Google Scholar]