- Visibility 495 Views
- Downloads 243 Downloads
- Permissions
- DOI 10.18231/j.jco.2025.014
-
CrossMark

Perceptions of patients regarding the cost of orthodontic treatment: Questionnaire based study
- Author Details:
-
 Rajiv Ahluwalia
Rajiv Ahluwalia
-
Mary Mathew
-
Tina Chugh *
-
Robin Mailk
-
Pradhumn Katara
Abstract
Background: Ensuring affordable orthodontic treatment is essential for promoting equitable access to dental care, emphasizing the significance of justice in addressing socio-economic disparities and fostering equal opportunities for individuals seeking orthodontic interventions. This study aims to investigate the perceptions of patients regarding the cost of orthodontic treatment and the factors influencing their views on affordability.
Materials and Methods: A semi-structured questionnaire was distributed to 116 participants undergoing orthodontic treatment to gather data on demographic information, personal experiences with orthodontic treatment, and attitudes toward the perceived cost of such treatment. The questionnaire was developed with input from orthodontic professionals and validated through pilot testing. Descriptive statistics including frequencies and percentages were calculated for all quantitative and categorical variables. Bivariate inferential analyses using chi-square tests were conducted to assess associations between categorical variables. Statistical significance was determined using a p-value cut-off of 0.05. P-values below 0.05 were considered statistically significant.
Results: The study showed that 96% of the participants were satisfied with the treatment. 94.0% felt that the treatment cost was justified by the duration of the treatment and the type of appliance. However, 49.1% of participants still felt the need for cost reduction. Patients with higher monthly income felt less need for cost reduction (p value < 0.001). There was an association between monthly income and the payment plan (p - 0.045), and between education and treatment satisfaction. (p-value = 0.018)
Conclusion: This questionnaire-based study sheds light on the diverse perceptions surrounding the cost of orthodontic treatment. Understanding these perspectives is crucial for healthcare professionals, policymakers, and stakeholders to develop strategies that enhance accessibility and affordability while addressing the broader implications of orthodontic care on individuals' well-being.
Background
Orthodontic treatment plays a crucial role in enhancing both the aesthetic appearance and functional aspects of the teeth and jaws, contributing to improved oral health, psychological well-being, and overall quality of life for patients.[1] Despite the evident benefits of orthodontic treatment, patients face challenges and barriers that influence their perceptions and satisfaction with the outcomes. Among these factors, the cost of treatment emerges as a critical consideration, with its variability determined by factors such as complexity of malocclusion, treatment duration, type of appliance, and experience of the orthodontist.[2], [3] The ethical foundation of healthcare emphasizes prioritizing patient welfare over financial considerations, aligning with George Merck's assertion that "Medicine is for the patient, not for profit. Profits will follow." However, the ethical landscape in orthodontics, much like in other healthcare professions, necessitates a delicate equilibrium between the pursuit of successful practices and the ethical responsibility to prioritize patient interests.
Understanding patients' perceptions of the cost becomes essential, as it can profoundly impact their motivation, expectations, and overall satisfaction with the treatment. Alabdullah et al. highlighted the influence of socio-demographic factors, including age, gender, education, income, and cultural background, on the perception of cost. [4] In particular, the financial burden associated with orthodontic treatment becomes pronounced in low - and middle-income countries, where public health systems may not cover or subsidize these services.[5], [6], [7] Moreover, this highlights the interconnection between cost perception, perceived value and benefits of treatment, willingness to pay, financial assistance-seeking behavior, and overall satisfaction and compliance.
Treatment cost affordability for all social classes is often rooted in the concept of justice and fairness in healthcare. This principle is often referred to as "distributive justice." Distributive justice involves the fair distribution of benefits and burdens in society, including affordable access to healthcare services.
One specific application of distributive justice in healthcare is the principle of equity. Equity in healthcare means that individuals should have equal affordable access to necessary medical treatments and services, regardless of their socioeconomic status. This principle acknowledges that people have different needs and resources but emphasizes the importance of ensuring that everyone has a fair opportunity to benefit from healthcare services.[8]
Patient autonomy, a fundamental principle in healthcare ethics, demands transparent communication regarding treatment costs and potential changes in the treatment plan. Informed consent is a key element of patient autonomy that empowers individuals to make decisions about their treatment after receiving comprehensive information. With the increase in patient awareness and involvement in every aspect of treatment decisions, it becomes paramount to assess their perceptions of orthodontic treatment costs, as it may affect the overall satisfaction of the patient.[6]
Despite advancements in orthodontic appliances and treatment options, little attention has been given to evaluate patients' perspectives on the evolving costs associated with these advancements. The current study aims to fill this gap by exploring how patients perceive the costs of orthodontic treatment. Understanding whether patients still find the costs prohibitive will contribute valuable insights for both practitioners and policymakers. Moreover, this research acknowledges the potential socio-economic burden on patients undergoing orthodontic treatment, an aspect that remains understudied. By evaluating patients' perceptions, satisfaction levels, and the correlation between these factors and the effectiveness of therapy, this study aims to shed light on the socio-economic implications of orthodontic treatment.
|
Details |
Response |
Number |
Percentage frequency |
|
Age |
<18 Years |
41 |
35.3 |
|
18-25 Years |
60 |
51.7 |
|
|
26-45 Years |
15 |
12.9 |
|
|
Gender |
Male |
49 |
42.2 |
|
Female |
67 |
57.8 |
|
|
Age |
No response |
6 |
5.2 |
|
School Going |
58 |
50.0 |
|
|
Undergraduate |
28 |
24.1 |
|
|
Graduate |
16 |
13.8 |
|
|
Postgraduate |
8 |
6.9 |
|
|
Reason for undergoing orthodontic treatment |
Forwardly placed teeth |
39 |
33.6 |
|
Malaligned teeth |
48 |
41.4 |
|
|
Jaw problem |
4 |
3.4 |
|
|
Facial look |
25 |
21.6 |
|
|
Recommendation for the treat ment |
Self-awareness |
65 |
56.0 |
|
Parents |
35 |
30.2 |
|
|
Peer |
3 |
2.6 |
|
|
Relatives |
10 |
8.6 |
|
|
Dentist/orthodontist |
3 |
2.6 |
|
|
Type of Orthodontic appliance |
Removable |
1 |
0.9 |
|
Aligners |
4 |
3.4 |
|
|
Fixed–metal braces |
95 |
81.9 |
|
|
Fixed–ceramic braces |
13 |
11.2 |
|
|
Fixed – self-ligating braces |
3 |
2.6 |
|
|
Monthly Income (per month) |
No response |
3 |
2.6 |
|
<10K |
42 |
36.2 |
|
|
10K-50K |
56 |
48.3 |
|
|
>50K |
15 |
12.9 |
|
Details |
Response |
Number |
Percentage frequency |
|
Total cost of treatment (in INR) |
<30,000 |
114 |
98.3% |
|
30,000-50,000 |
2 |
1.7% |
|
|
Payment Plan |
One-time complete payment |
28 |
24.1% |
|
Payment in two installments |
16 |
13.8% |
|
|
Monthly payment |
58 |
50.0% |
|
|
Once in two months |
3 |
2.6% |
|
|
Irregular Schedule |
11 |
9.5% |
|
|
Methods of Orthodontic Treatment Payment |
Government service/free of cost/discounts applicable |
2 |
1.7% |
|
Self pay |
107 |
92.2% |
|
|
Insurance |
7 |
6.0% |
|
Details |
Response |
Number |
Percentage frequency |
|
Major Barriers Preventing Individuals from Undergoing Orthodontic Treatment |
High cost |
77 |
66.3 |
|
Long duration |
45 |
38.7 |
|
|
Fear of pain |
13 |
11.2 |
|
|
Fear of extraction |
9 |
7.5 |
|
|
Treatment Satisfaction |
Yes |
111 |
95.7% |
|
No |
5 |
4.3% |
|
|
Perception of Treatment Cost Justification to treatment Time Duration, and Appliance Type |
Yes |
109 |
94.0% |
|
No |
7 |
6.0% |
|
|
Perception of need for treatment cost reduction |
Yes |
69 |
59.5% |
|
No |
47 |
40.5% |
|
|
Perspectives on the Inclusion of Orthodontic Treatment Costs in Dental Insurance |
Yes |
61 |
52.6% |
|
No |
12 |
10.3% |
|
|
May be |
43 |
37.1% |
|
Materials and Methods
This cross-sectional study was conducted on 145 patients undergoing orthodontic treatment at various orthodontic clinics and centers in NCR Delhi. Twenty-nine of patients did not fill the questionnaire completely (response rate-0.80%). Thus, 116 patients were included in the study. Individuals without a history of orthodontic treatment and other corrective orthognathic surgeries were excluded.
The semi-structured questionnaire was developed based on a comprehensive literature review and input from orthodontic professionals, ensuring its content validity. Pilot testing with a small group of participants was conducted to assess clarity, comprehensibility, and relevance, with feedback used to refine the questionnaire for enhanced face validity. To ensure reliability, the questionnaire was designed to be clear, unambiguous, and consistent in its wording. Participants were provided with instructions to minimize response errors, and trained research assistants administered the questionnaire to ensure consistency in data collection procedures. The details included demographic information, the reason for seeking and undergoing orthodontic treatment, the type of appliance they chose for the treatment on the cost of the treatment and the justified cost towards the treatment. The study commenced after obtaining approval from the Institutional Ethics Committee, Santosh deemed to be University (IEC No. F. No. SU/2021-22). A written informed consent was obtained from the participants.
The data for this study was collected and entered in Microsoft Excel 2010 for initial data management and cleaning. Once the data set was finalized, it was imported into Stata MP version 17 for statistical analysis. Descriptive statistics including frequencies and percentages were calculated for all qualitative and categorical variables. Graphical representations such as pie charts and histograms were produced for key variables to allow for easier interpretation of results. Bivariate inferential analyses using chi-square tests were conducted to assess associations between categorical variables. Statistical significance was determined using a p-value cut-off of 0.05. P-values below 0.05 were considered statistically significant, indicating an association between the variables. P-values above 0.05 were considered statistically insignificant, signifying no detectable association. The results of the descriptive and inferential analyses were presented using appropriate tables and graphs.
Results
The presented data provides insights into the perception of the cost of orthodontic treatment among a sample of 116 individuals. The study includes demographic information, sources of recommendations, and the influence of socio-economic factors on perceptions of treatment cost.
The majority of respondents were in the 18-25 age group (51.7%), with a slight female predominance (57.8%). Education levels varied, with a significant portion being school-going individuals (50.0%). Misaligned teeth (41.4%) and forwardly placed teeth (33.6%) were the primary reasons for seeking orthodontic treatment. Jaw problems (3.4%) and concerns about facial appearance (21.6%) were also cited as reasons. Self-awareness (56.0%) was the most common source of recommendation for orthodontic treatment, followed by parents (30.2%). 81.9% of participants chose fixed metal appliance for treatment. Most respondents reported a monthly income of less than 50,000 INR (87.1%). ([Table 1])
98.3% of participants had their treatment cost less than Rs. 30,000. The preferred payment plan was monthly payments (50.0%) (p < 0.045). 92.2% of patients paid themselves for the treatment. ([Table 2])
The participants felt that the most common barrier for people to not undergo orthodontic treatment is the high cost (66.3%) followed by the fear of long duration (38.7%). Other reasons included fear of pain (11.2%) and fear of extraction (7.8%). The vast majority (95.7%) were satisfied with the treatment progress. 94.0% felt that the treatment cost was justified by the duration of the treatment and type of appliance. However, 59.5% of patients perceived treatment costs to be high, and felt the need for cost reduction. 52.6% of patients felt that the treatment cost should be covered under dental insurance. ([Table 3])
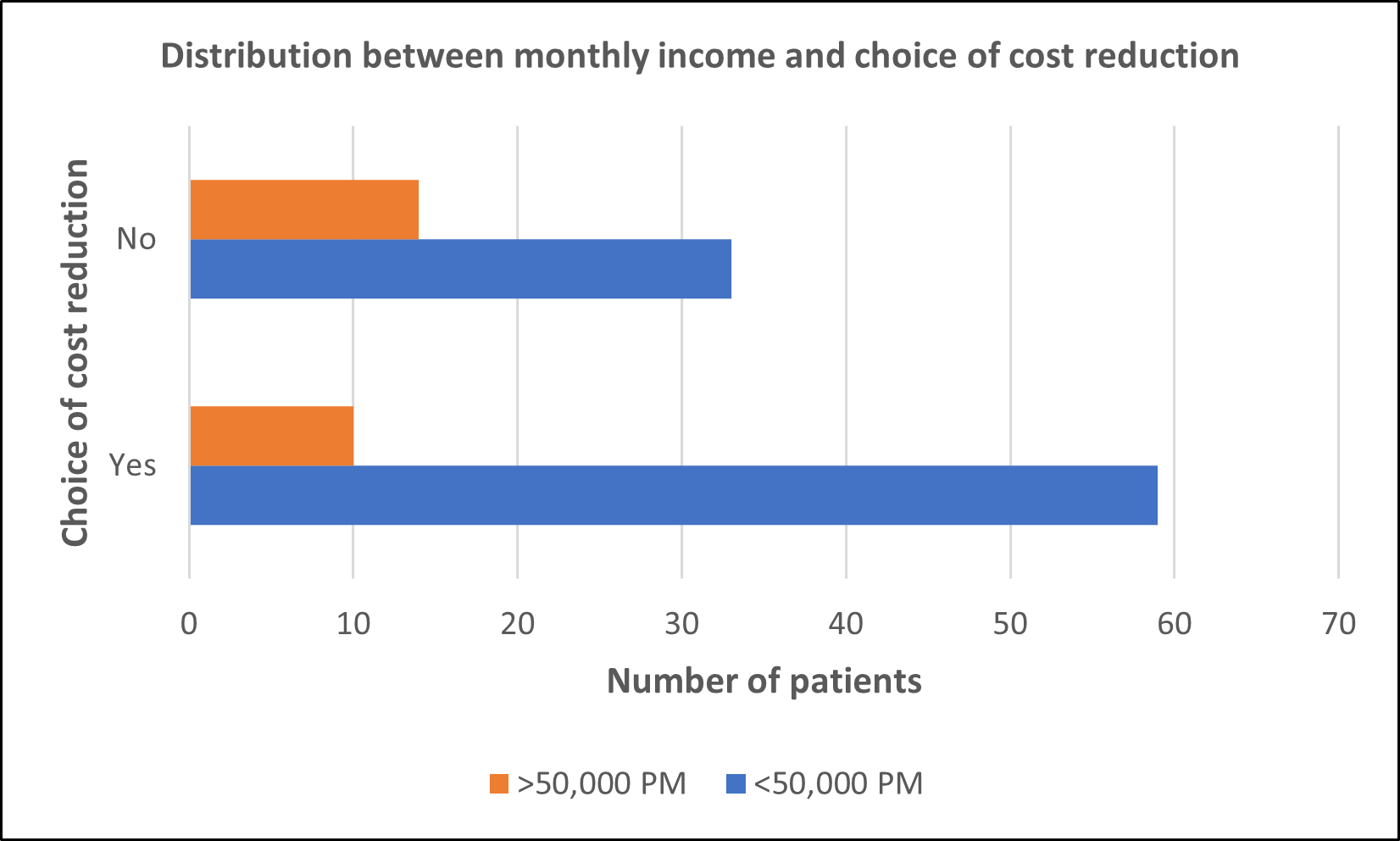
An association was found between monthly income and the opinion regarding the need for cost reduction in orthodontic treatment. (p-value - 0.046). Patients with higher monthly income felt less need to cost reduction compared to patients with less than 50K. ([Figure 1])
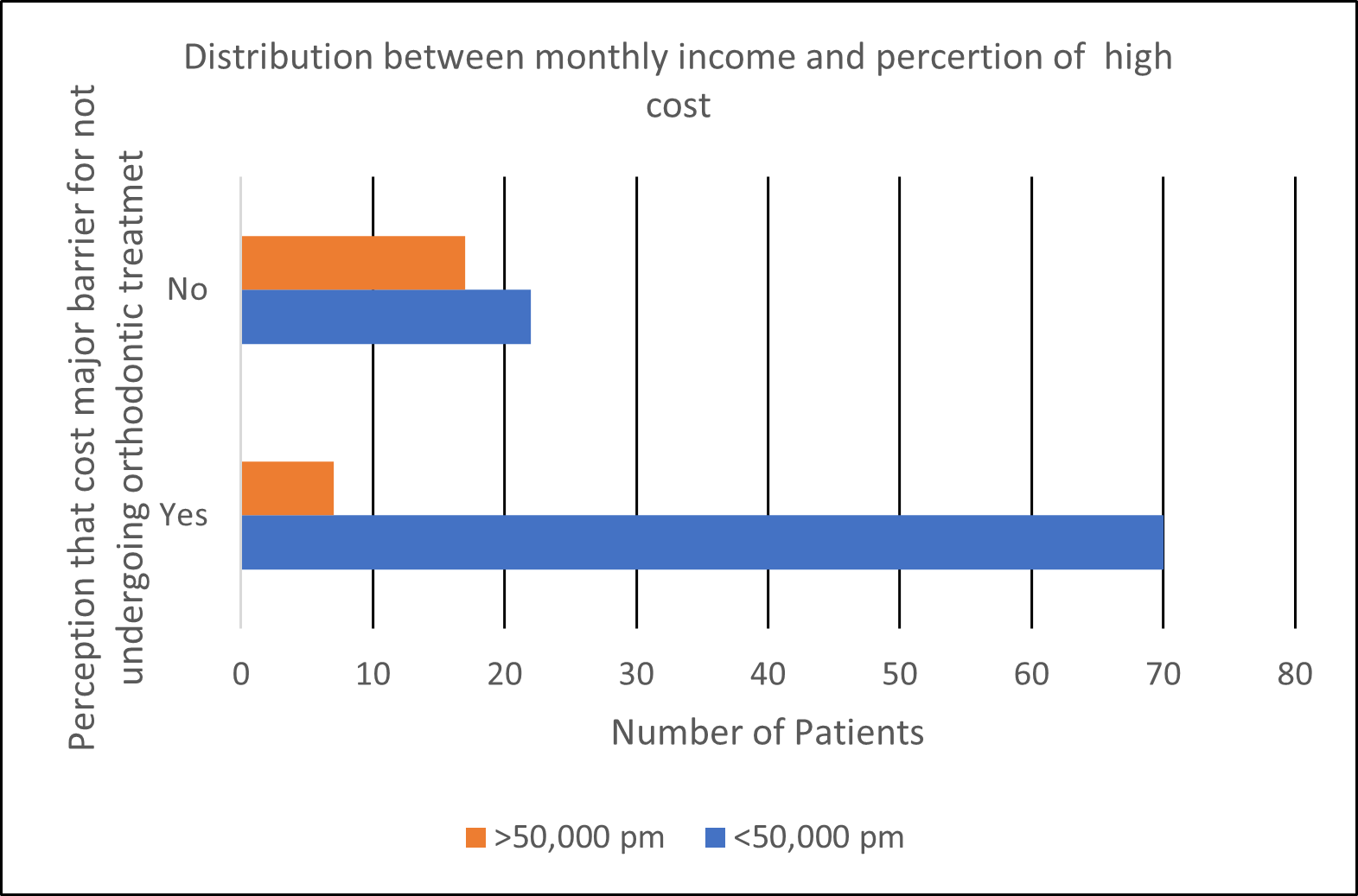
No association was found between monthly income and the perception that high treatment cost being the major barrier for not undergoing orthodontic treatment. (p-value = 0.986)*([Figure 2])
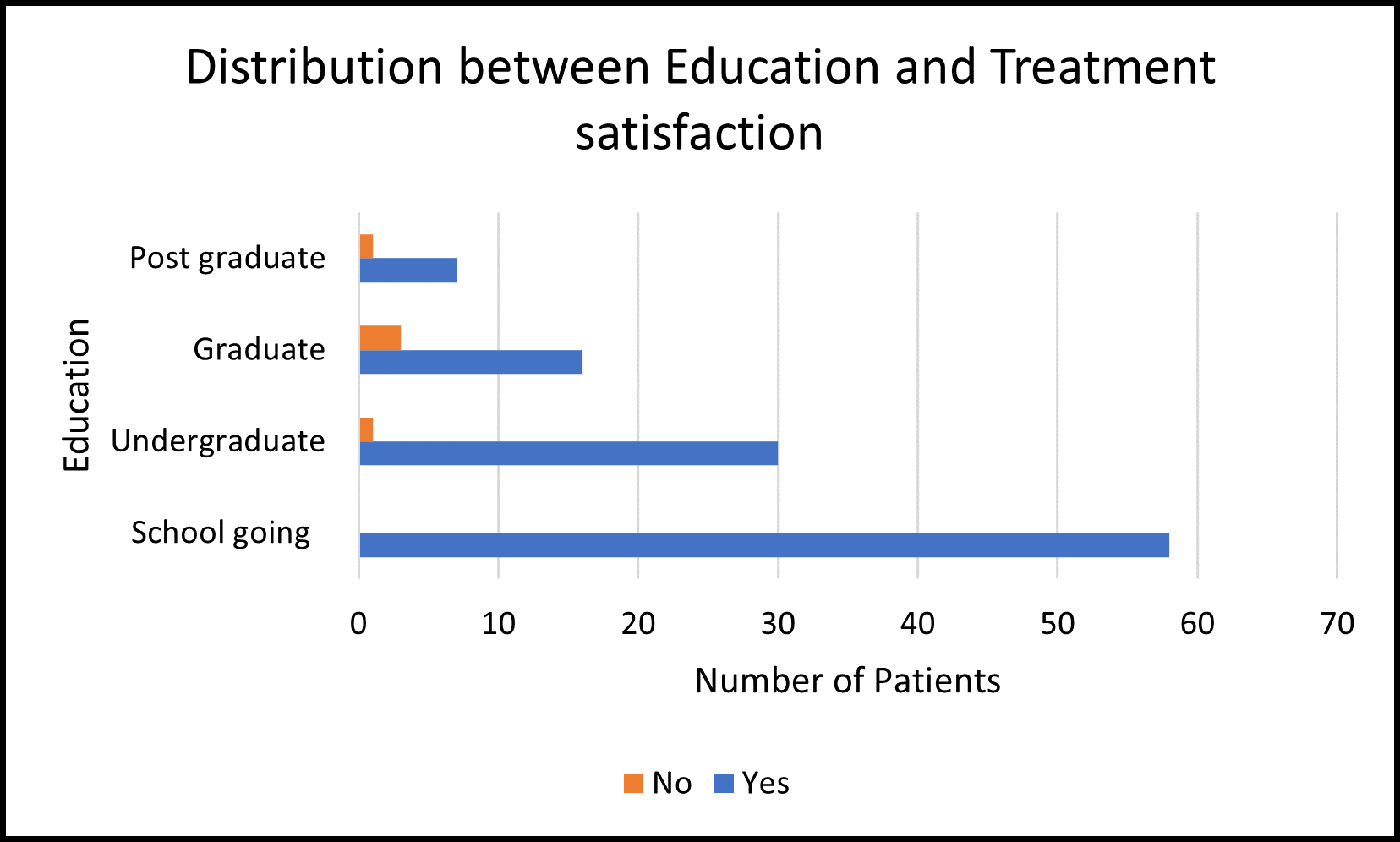
The majority of respondents across all education levels seem to be satisfied with the treatment progress. A significant association was found between education levels and treatment satisfaction (p-value of 0.018) implying that individuals with different education levels have varying degrees of satisfaction with the treatment progress. (Figure 3)
Discussion
The presented study on the perception of the cost of orthodontic treatment provides valuable insights into the factors influencing individuals' decisions regarding orthodontic care. The study indicates a predominant representation of individuals in the 18-25 age group, aligning with existing literature that highlights a higher prevalence of orthodontic treatment during adolescence and early adulthood due to high prevalence of low self-concept in adolescents with dental malocclusion. [9], [10] Peres et al. [11] have suggested that adolescents reported pleasant esthetics as an important factor for psychosocial well-being and, in general, that orthodontic treatment is accepted as an important part of the health service, especially due to the psychological impact of malocclusion on self-esteem. The gender distribution in the study is consistent with previous research, which often reports a slightly higher percentage of females seeking orthodontic care. [12], [13] Breece and Nieberg, and Khan and Horrocks also observed higher female patients when compared to males. [14], [15] This could be due to higher esthetic standards in females.
It is noteworthy that a substantial proportion of the patients seeking orthodontic treatment were in the school-going age group. This demographic insight suggests that the demand for orthodontic treatment in children appears to be strongly influenced by parental factors, with parental influence emerging as the most crucial predictor. [16] It could be due to the desire for their child to have an aesthetically pleasing appearance. The findings highlight that a significant proportion of individuals seeking orthodontic care were motivated by concerns related to the alignment and positioning of their teeth, were in line with study done by Shaw et al. [17] and Feldons et al. [18] In the present study, health and function did not appear to be a key motivational factor to seek treatment. The study emphasizes self-awareness as a primary source of recommendation, diverging from some existing literature that often highlights the role of dentists and orthodontists in recommending treatment.[19] Parents' influence on the decision-making process aligns with the family-centered nature of orthodontic care decisions, as reported in various studies.[16], [20] This could potentially drive by a motivation to align with societal norms. The preference for fixed metal braces among the majority of patients is likely influenced by cost considerations. The high prevalence of fixed-metal braces in this study contrasts with the growing popularity of aligners reported in recent literature.[21] This may reflect regional variations or the specific characteristics of the study population.
Various payment methods are typically implemented to streamline the collection of treatment fees and appeal to diverse financial segments, aligning with findings by Walley et al.[22] indicating that a key factor in selecting a dental office is the availability of favorable payment plans, ranked second only to dentist referrals. The majority of patients, in this context, opt for monthly payment plans.
The major barrier reported in this study, namely the high cost, resonates with previous literature emphasizing financial considerations as a significant deterrent to orthodontic treatment. [23], [24] Fear of pain and extraction, though less frequently cited, aligns with the broader literature on patient concerns and apprehensions regarding orthodontic procedures.[25]
The data indicates that the cost remains a significant barrier to orthodontic treatment, particularly for individuals with lower incomes and lower education levels. A similar finding was observed by Chambers and Zitterkopf.[23] This emphasizes the need for initiatives to make orthodontic care more affordable, such as subsidies, insurance coverage, or payment plans.
However, the high treatment satisfaction rate and the perception of cost justification among those undergoing treatment suggest that individuals value the benefits of orthodontic care. Efforts to increase awareness about these benefits and address misconceptions about treatment costs may contribute to greater acceptance of orthodontic care. Additionally, the findings highlight the importance of considering socio-economic factors in public health policies related to orthodontic care access is in line with Article 14, Universal Declaration on Bioethics and Human Rights.[26]
The association between monthly income and the perception of high treatment costs is consistent with previous research indicating the impact of socio-economic status on orthodontic treatment affordability.[6] The study's findings on the belief that treatment costs should be reduced advocates measures to enhance affordability.
The association between education level and the perception of treatment progress introduces a novel aspect. While literature often explores socio-economic status, this study suggests that educational background may also influence patients' understanding and satisfaction with treatment outcomes.
The study raises ethical considerations regarding the affordability of orthodontic treatment. While satisfaction levels were high, there is a notable proportion (40.5%) who believe that treatment costs should be reduced. Furthermore, the question whether orthodontic treatment costs should be covered under dental insurance received mixed responses, highlighting the ethical dilemma of balancing affordability and sustainability.
This study aims to explore the multifaceted ethical dimensions of orthodontic treatment costs from the perspective of patients. By delving into patients' perceptions, we seek to uncover potential challenges and inequities in the orthodontic care landscape. The ethical principles of autonomy, beneficence, non-maleficence, and justice underpin our commitment to conducting this research. We aim to respect patients' autonomy by understanding their views, promote beneficence by identifying ways to enhance the affordability of orthodontic care, and prevent non-maleficence by minimizing the financial burden associated with treatment.
The study is limited by its cross-sectional design, providing a snapshot of perceptions at a specific point in time. Self-reporting bias may be present in participants' responses. Further studies can be done to employ a longitudinal approach to capture dynamic changes in patient perceptions over time. Additionally, incorporating objective measures alongside self-reporting could mitigate potential bias.
Conclusion
The study contributes valuable data to the existing body of literature on orthodontic treatment perceptions. The findings emphasize the need for targeted interventions to address financial barriers, considering both income levels and educational backgrounds. Further studies can be done to explore the psychological aspects of cost perception, such as the influence of perceived benefits, self-esteem, and social comparison and investigate how these factors affect individuals' willingness to invest in orthodontic treatment.
Source of Funding
None.
Conflict of Interest
None.
References
- Imani M, Jalali A, Dinmohammadi M, Nouri P. The Effect of Orthodontic Intervention on Mental Health and Body Image. Open Access Maced. J Med Sci. 2018;17(6):1132-7. [Google Scholar]
- Germa A, Kaminski M, Nabet C. Impact of social and economic characteristics on orthodontic treatment among children and teenagers in France. Commun Dent Oral Epidemiol. 2010;38(2):171-80. [Google Scholar]
- Bresnahan B, Kiyak H, Masters S, Mcgorray S, Lincoln A, King G. Quality of life and economic burdens of malocclusion in U.S. patients enrolled in Medicaid. J Am Dent Assoc. 2010;141(10):1202-12. [Google Scholar]
- Alabdullah J, Saltaji H, Abreu L. Factors affecting patients’ adherence to orthodontic appointments. BMC Oral Health. 2018;18(1). [Google Scholar]
- Ghonmode S, Shrivastava S, Kadaskar A, Bapat S. Socioeconomic burden of orthodontic treatment: a systematic review. Med Pharm Rep. 2023;96(2):154-63. [Google Scholar]
- Chaturvedi M, Ahluwalia R, Chugh T, Yadav D, Gupta M, Kaur P. Affordability of orthodontic treatment: A step towards the economic evaluation. J Pharm Neg Result. 2022;13(6):1104-13. [Google Scholar]
- Alam M, Alqahtani N, Alqahtani S. Orthodontic treatment need and demand among 12-15 year-old Saudi schoolchildren. J Orthod Sci. 2018;7(1):1-7. [Google Scholar]
- Beauchamp T, Childress J. Principles of Biomedical Ethics. Emer Med . 2019;17(2):283-306. [Google Scholar]
- Perillo L, Esposito M, Caprioglio A, Attanasio S, Santini A, Carotenuto M. Orthodontic treatment need for adolescents in the Campania region: the malocclusion impact on self-concept. Patient Prefer Adher. 2014;8:353-59. [Google Scholar]
- Trulsson U, Strandmark M, Mohlin B. A qualitative study of teenagers’ decisions to undergo orthodontic treatment with fixed appliance. J Orthod. 2002;29(3):197-204. [Google Scholar]
- Peres S, Goya S, Cortellazzi K. Self-perception and malocclusion and their relation to oral appearance and function. Cien Saude Colet. 2011;16(10):4059-66. [Google Scholar]
- Pabari S, Moles D, Cunningham S. Assessment of motivation and psychological characteristics of adult orthodontic patients. Am J Orthod Dentofac Orthop. 2017;152(2):247-55. [Google Scholar]
- Saccomanno S, Saran S, Laganà D, Mastrapasqua R, Grippaudo C. Motivation, Perception, and Behavior of the Adult Orthodontic Patient: A Survey Analysis. Biomed Res Int. 2022. [Google Scholar]
- Breece G, Nieberg L. Motivations for adult orthodontic reatment. J Clin Orthod. 1986;20(3):166-71. [Google Scholar]
- Khan R, Horrocks E. A study of adult orthodontic patients and their treatment. Brit J Orthod. 1991;18(3):183-94. [Google Scholar]
- Brumini M, Slaj M, Katic V, Pavlic A, Zrinski T, Spalj M. Parental influence is the most important predictor of child's orthodontic treatment demand in a preadolescent age. Odontology. 2020;108(1):109-16. [Google Scholar]
- Shaw W, Obrien K, Richmond S. Quality control in orthodontics: factors influencing the receipt of orthodontic treatment. Br Dent J. 1991;170(2):66-74. [Google Scholar]
- Feldens C, Nakamura E, Tessarollo F, Closs L. Desire for orthodontic treatment and associated factors among adolescents in Southern Brazil. Angle Orthod. 2015;85(2):224-56. [Google Scholar]
- Aldrees A, Tashkandi N, Alwanis A, Alsanouni M, Al-Hamlan N. Orthodontic treatment and referral patterns: A survey of pediatric dentists, general practitioners, and orthodontists. Saudi Dent J. 2015;27(1):30-9. [Google Scholar]
- Kazancı F, Aydoğan C, Alkan �. Patients’ and parents’ concerns and decisions about orthodontic treatment. Korean J Orthod. 2016;46(1):20-6. [Google Scholar]
- Tamer �, Öztaş E, Marşan G. Orthodontic Treatment with Clear Aligners and The Scientific Reality Behind Their Marketing: A Literature Review. Turk J Orthod. 2019;32(4):241-6. [Google Scholar]
- Walley E, Silberman S, Tuncay O. Patient and parent preferences for orthodontic practices. Clin Orthod Res. 1999;2(3):110-33. [Google Scholar]
- Chambers D, Zitterkopf J. How people make decisions about whether or not to seek orthodontic care: Upstream in the treatment chain. Am J Orthod Dentofac Orthop. 2019;155(6):826-31. [Google Scholar]
- Gutierrez T. Overcoming barriers to orthodontic treatment in the United States. Dent Hypotheses. 2016;7(2):70-2. [Google Scholar]
- Chowj J, Cioffi I. Pain and orthodontic patient compliance: A clinical perspective. Semin Orthod. 2018;24(2): 242-7. [Google Scholar]
- . Universal Declaration on Bioethics and Human Rights. . . [Google Scholar]