- Visibility 260 Views
- Downloads 48 Downloads
- Permissions
- DOI 10.18231/j.jco.2025.009
-
CrossMark

Assessment of cortical plate thickness and bone density of mandibular symphyseal region in subjects having skeletal Class III malocclusion with different facial types – A CBCT study
- Author Details:
-
 Devanshi Churiwal *
Devanshi Churiwal *
-
Jitendra Bhagchandani
-
Vaibhav Vashishta
-
Ayushi Singh
-
Stuti Raj
-
Tushant Rastogi
Abstract
Background: The study used CBCT to analyze mandibular symphyseal bone thickness and density in Skeletal Class III subjects with different vertical facial patterns. It found higher cortical bone thickness in Normodivergent and higher bone density in Hypodivergent subjects, emphasizing the importance of careful orthodontic treatment to avoid complications related to reduced bone density and cortical thickness.
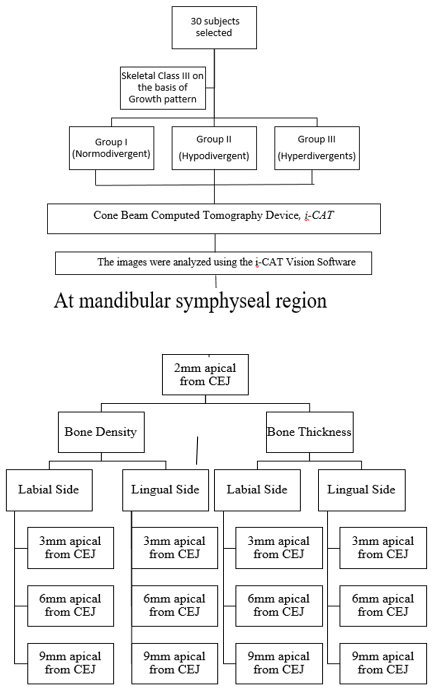
Materials and Methods: CBCT images of 30 skeletal Class III subjects were evaluated. Class III subjects were divided by mandibular plane angle: Hyperdivergent (SN–MP > 34o), Normodivergent (SN–MP – 32o), and Hypodivergent (SN–MP < 30o) groups. Buccolingual cortical bone thickness and bone density was measured using CBCT images of mandibular incisors at alveolar crest and 3, 6 and 9 mm apical levels. Shapiro Wilk test, Bonferroni post-hoc test, and Pearson correlation analysis were used for statistical significance.
Results: The mean cortical bone thickness of the mandibular symphyseal region was highest in Normodivergent subjects (Group I) and lowest in Hyperdivergent subjects (Group III). Group II subjects with a Hypodivergent growth pattern had the highest mean bone density, with the lowest reported in Normodivergent subjects on the labial side and Hyperdivergent subjects on the lingual side. However, differences in bone density among groups were statistically insignificant.
Conclusions: Careful orthodontic treatment in Skeletal Class III malocclusion, especially with Hyper-divergent facial types, is crucial to prevent root issues due to reduced bone density. Bracket adjustments are essential for optimal outcomes by ensuring proper root placement within cancellous bone.
Introduction
Orthodontics is a dynamic field of dentistry that continually seeks to enhance its diagnostic as well as treatment planning capabilities. Excellent cosmetic dental and facial esthetics can be achieved with orthodontic therapy but, periodontal problems such as fenestration, bone dehiscence, vertical bone loss, and gingival recession also occur during its course.[1]
Skeletal Class III malocclusion, characterized by a prognathic mandible relative to the maxilla, poses distinct challenges in orthodontic treatment. When undergoing orthodontic camouflage treatment, the patient’s lower anterior tooth movements should be closely monitored to achieve a positive overjet by lingual tipping of lower incisors. Hence correcting the anterior crossbite is among the most challenging tooth movements in orthodontic therapy for skeletal Class III subjects.[2]
Alveolar bone remodeling and periodontal ligament enlargement are the mechanisms by which teeth move.[3] When teeth are moved beyond the biological limits of the alveolar bone, it undergoes root resorption, gingival recession, fenestration, and alveolar bone loss. [4]
The mandibular symphyseal region is a focal point for orthodontic interventions and it requires a closer examination due to its involvement in the mandibular positioning and stability. The cortical plates of the alveolar bone and the mandibular symphysis at the root apex act as anatomical barriers since there is less bone remodeling in this region than in the alveolar crest or mid radicular region.[5], [6]
Understanding the cortical plate thickness and bone density in this region is essential, as it can influence treatment mechanics, anchorage considerations, and the overall success of orthodontic interventions in subjects with Skeletal Class III malocclusion.
Among the myriad of factors influencing the treatment outcome, the cortical plate thickness and bone density of the mandibular symphyseal region play a pivotal role. Therefore, this research endeavours to undertake a comprehensive investigation into these aspects, using CBCT and focusing specifically on subjects exhibiting Class III skeletal malocclusion with different facial types.
The study aimed to use CBCT scans of Class III skeletal jaw base with different facial patterns at the mandibular symphyseal region at different levels from the CEJ of mandibular central incisors, to assess the association between the width of synphysis and densities at lingual and labial surfaces of the mandibular anterior teeth.
A judiciously selected sample representing diverse facial types underwent comprehensive radiographic analysis and subsequent measurements of cortical plate thickness and bone density, were performed.
Materials and Methods
The study was conducted on 30 subjects within the age group of 18-30 years who reported to the Department of Orthodontics and Dentofacial Orthopedics, SPPGIDMS, Lucknow for fixed orthodontic treatment.
Skeletal Class III subjects were chosen for the present study based on their ANB angle, Beta angle, Wits appraisal, and Yen angle. Samples were divided into 3 groups based on their facial types.
Group I (n=10) - Skeletal Class III subjects with normo-divergent growth pattern, based on Lower Gonial angle: 70o-75o, Y-axis: 66o, SN-Go-Gn, Mandibular plane angle: 32o
Group II (n=10) - Skeletal Class III subjects with hypo divergent growth pattern, based on Lower Gonial angle < 70o, Y-axis < 66o, SN-Go-Gn, Mandibular plane angle < 30o
Group III (n=10) - Skeletal Class III subjects with hyper divergent growth pattern, based on Lower Gonial angle > 70o, Y-axis > 66o, SN-Go-Gn, Mandibular plane angle > 34o.
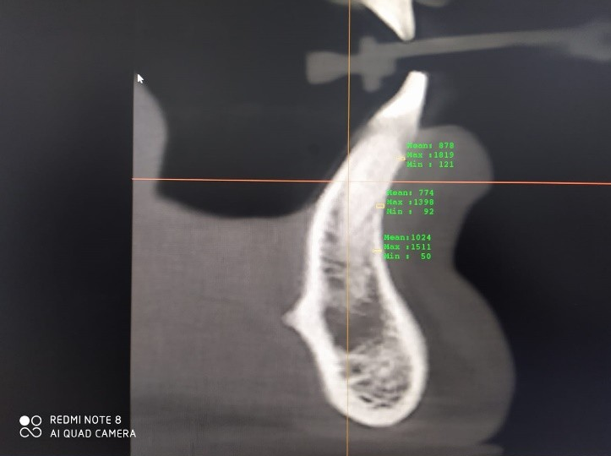
Cone Beam Computed Tomography (CBCT i-CAT), was utilized to scan selected subjects in the region of the mandibular symphysis. Patients undergoing Cone Beam Computed Tomography (CBCT) were instructed to remove any metallic items from their heads and necks, such as jewelry, spectacles, and hairpins. They were then positioned facing the CBCT machine while standing. Proper head positioning on Frankfort's horizontal plane was ensured using the localizer. Once the patients were oriented correctly, the gantry with sensors rotated around the patient's head to initiate scanning as per the equipment's instructions. Subsequently, the digital image appeared on the monitor for further analysis and assessment.
The scanning protocol involved creating an axial plane positioned 2 mm apical to the cemento-enamel junction of the mandibular incisors. From this axial plane, three transverse sections were obtained. The assessment focused on measuring the thickness of the labial and lingual cortical plates as well as bone density at three different levels: 3 mm, 6 mm, and 9 mm apical from the alveolar crest for all the subjects.
Results
The study was conducted on 30 subjects having skeletal Class III with different facial types, which were then subjected to Statistical Analysis using Statistical Package for Social Sciences (SPSS) software Version 21. Shapiro Wilk Test was used for analysis of normality for data distribution while inferential statistics were calculated using one way ANOVA test along with Post Hoc Turkey’s test. Level of statistical significance was set at 0.05.
|
Bone thickness on Labial side |
||||||
|
|
N |
Mean |
Std. Deviation |
P value |
Post hoc pau"\vtse companson |
|
|
DI |
Grl |
10 |
.52600 |
.120573 |
0.077, NS |
NA |
|
Grll |
10 |
.51800 |
.118491 |
|||
|
Gr ill |
10 |
.42300 |
.079380 |
|||
|
02 |
Grl |
10 |
.75100 |
.250076 |
0.597, NS |
NA |
|
Gr II |
10 |
.68500 |
.138624 |
|||
|
Gr ill |
10 |
.65750 |
.223100 |
|||
|
03 |
Grl |
10 |
l.10450 |
.261900 |
0.406, NS |
NA |
|
Gr II |
10 |
l.06300 |
.218901 |
|||
|
Gr ill |
10 |
.97300 |
.170036 |
|
Bone thickness on lingual side |
||||||
|
|
N |
Mean |
Std. Deviation |
P value |
Post hoc pan-w:tse c01npans011 |
|
|
DI |
Gr l |
10 |
.84200 |
.188686 |
0.507, NS |
A |
|
Gr II |
10 |
.82450 |
.515473 |
|||
|
GFIII |
10 |
.67100 |
.281995 |
|||
|
02 |
Gr l |
10 |
1.15850 |
.481837 |
0.315, NS |
A |
|
Gr II |
10 |
.98900 |
.197833 |
|||
|
Gr III |
10 |
.90100 |
.393558 |
|||
|
03 |
Gr! |
10 |
1.54250 |
.438015 |
0.06 NS |
NA |
|
Gr II |
10 |
1.36395 |
.212176 |
|||
|
Gr III |
10 |
1.09050 |
.510596 |
|
Bone density on Labial side |
|||||||
|
|
|
Mean |
Std. Deviation |
P value |
Post hoc pairwise companson |
||
|
01 |
GrI |
10 |
472 .0000 |
189.20682 |
0..433 NS |
NA |
|
|
Gr IT |
10 |
583.4500 |
250 .91371 |
||||
|
Gr ill |
10 |
497.1500 |
141.28833 |
||||
|
02 |
Gr I |
10 |
642.5000 |
233.06353 |
0 |
.. 118, NS |
NA |
|
|
|||||||
|
Gr IT |
10 |
824.6000 |
234.90 197 |
||||
|
Gr ill |
10 |
663.1000 |
140.02972 |
||||
|
03 |
Gr I |
10 |
955.0000 |
208.35387 |
0..178 NS |
NA |
|
|
Gr II |
10 |
1111.4500 |
198.02812 |
||||
|
Gr ill |
10 |
979.7500 |
180.08119 |
|
Bone density on Lingua] side |
||||||
|
|
N |
Mean |
Std. Deviation |
P value |
Post hoc pa11'\v1.se companson |
|
|
DI |
GrI |
10 |
1113.3000 |
236.98338 |
0..633, NS |
1 A |
|
|
||||||
|
Gr II |
10 |
1125.8500 |
197.08205 |
|||
|
Gr III |
10 |
1033.3000 |
260.45763 |
|||
|
D2 |
GrI |
10 |
1201.0500 |
25l.92883 |
0..151, NS |
A |
|
Gr II |
10 |
l34L9500 |
119.47093 |
|||
|
Gr III |
10 |
1126.1500 |
315.63481 |
|||
|
D3 |
GrI |
10 |
1380.2000 |
184.21548 |
0..140, NS |
A |
|
Gr II |
10 |
1443.7500 |
96.78764 |
|||
|
Gr III |
10 |
1276.5500 |
240.156]4 |
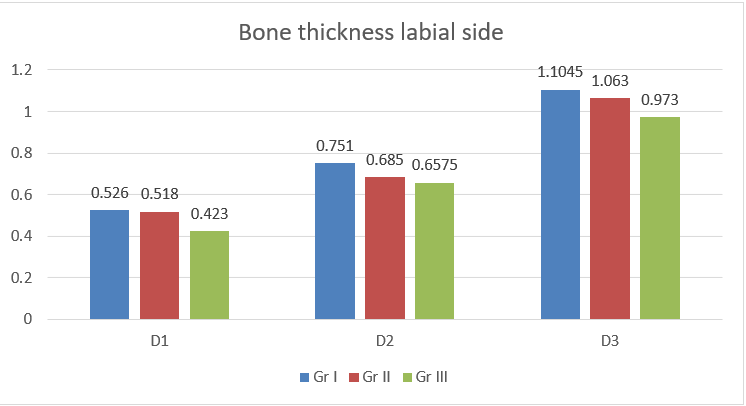
Group I participants with Normodivergent growth patterns had the maximum labial bone thickness, while those with Hyperdivergent patterns had the minimum, with insignificant statistical differences among groups. ([Table 1], [Figure 3])
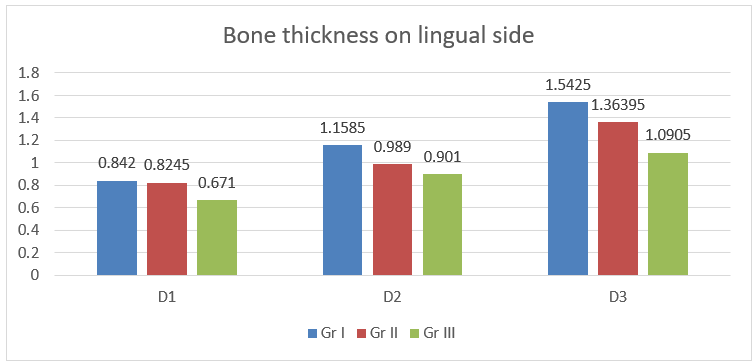
Similarly, on the lingual side, Group I individuals with Normodivergent growth patterns had the highest bone thickness, while those with Hyperdivergent patterns had the lowest, but differences were not statistically significant. ([Table 2], [Figure 4])
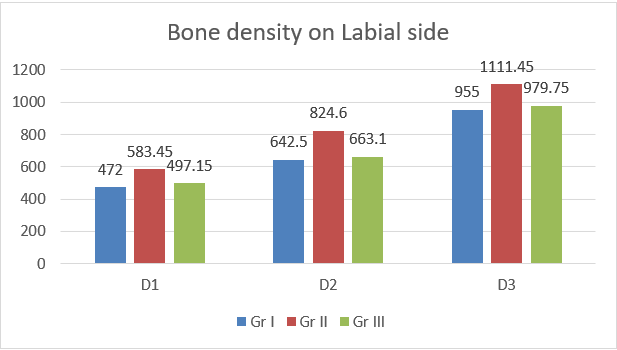
Group II individuals with Hypodivergent growth patterns had the highest labial bone density on teeth 31 and 41, while Group I individuals with Normodivergent growth patterns had the lowest, but differences were not statistically significant.([Table 3], [Figure 5])
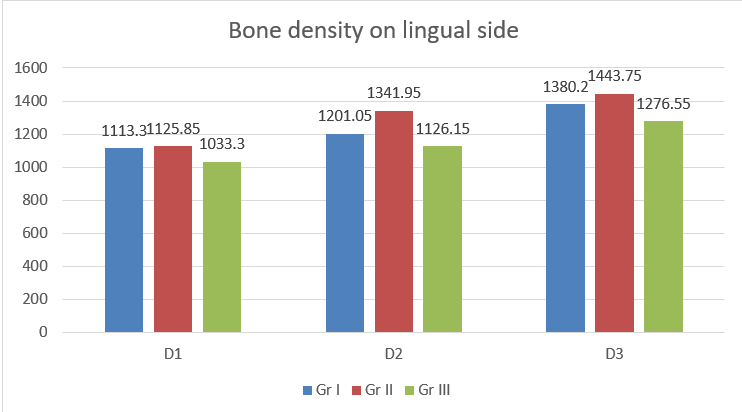
On the lingual side, Group II participants with Hypodivergent growth patterns had the highest bone density at 3mm. In contrast, Group III with Hyperdivergent patterns had the lowest, yet the differences were not statistically significant. ([Table 4], [Figure 6])
Discussion
The assessment of facial patterns is crucial as the course of therapy and prognosis varies in different facial patterns of growth.[7] According to Karlsen,[8] subjects between the age group 6-12, show entirely distinct patterns of craniofacial development, with high and low angle values. According to Isaacson et al.,[9] face growth advances along a vector consisting of varying proportions of vertical downward growth and horizontal forward growth in relation to the cranial baseline.[10]
Morphology of Symphysis has been utilized to predict the direction of mandibular growth.[11] Bjork[12] published an account of various structural arrangements found in extreme forms of the mandibular rotators. He discovered that a forward inclination of the condylar head and an increased curvature of the mandibular canal relative to the mandibular contour were related to a forward mandibular rotation.
According to Moshfeghi M et al.[13] certain symphyseal measurements varied considerably between categories. There were no discernible variation in the height of the symphysis between the Class III horizontal and vertical groups, and the Class III vertical groups had a greater height. Concerning to the symphysis depth, Class III horizontal growers exhibited the maximum depth, whereas Class II vertical growers had a minimal depth.
Bone density
In our present study, Group II (Hypodivergent Subjects) reported maximum bone density on the labial sides, at all 3 levels i.e. 3mm (583.4500 Hu), 6mm (824.6000 Hu) and 9mm (1111.4500 Hu) as well as on the lingual sides at 3mm (1125.8500Hu) 6mm (1341.9500 Hu) and 9mm (1443.7500 Hu) apical from the alveolar crest whereas, Group I subjects (Normodivergent subjects) showed minimum bone density on the labial sides at all 3 levels i.e. 3mm (472.0000 Hu); 6mm (642.5000 Hu) and 9mm (955.0000 Hu) while Group III (Hyperdivergent subjects) reported minimum bone density on the lingual sides at all 3 levels i.e. 3mm (1033.3000Hu), 6mm (1126.1500Hu) and 9mm (1276.5500Hu) apical from the alveolar crest.
Similar outcomes were seen in a prior investigation of Gousman et al [14] where the cancellous bone density were found to be higher in Skeletal Class III hypodivergent subjects when compared with different facial types. Killaridis [15] reported that hypodivergent skeletal pattern exhibits greater masticatory muscle force as compared with hyperdivergent skeletal patterns.This partially explains the underlying reason behind the increased muscle strength seen in hypodivergent cases.
Bone thickness
In the present study, the thickness of the cortical bone were compared at 3mm, 6mm, and 9mm apical from the CEJ in the symphyseal region with skeletal Class III subjects. Group I (Normodivergent subjects) reported maximum bone thickness of the mandibular incisor's labial and lingual surfaces followed by Group II (Hypodivergent), and the least bone thickness were found in Group III (Hyperdivergent) subjects. The thickness of the alveolar bone in this investigation at 3mm (0.42mm) and 6mm (0.65mm) apical to the CEJ were found to be decreased on the labial aspect and had the lowest value in the Class III high angle group. This suggested that in skeletal Class III high angle individuals, caution must be used when decompensating mandibular anterior teeth during pre-surgical orthodontics. Careful evaluation of the periodontal health at the mandibular anterior region during the retention phase would be required since the mandibular incisors in the Class III high-angle group were much more lingually placed and the alveolar bone were significantly weaker. The above findings were similar to those of Gaffuri et al.[16] and Kuitert et al. [17]
Similar results were found in a study by Sadek et al.[18] who used CBCT to examine variations in skeletal and alveolar dimensions among participants with varying vertical face dimensions. They concluded that the anterior maxilla and nearly every location in the lower jaw showed thinner alveolar thickness within the group comprising of high mandibular plane angle.
A systematic review conducted by Silviana NM[19] showed a statistically strong correlation between Alveolar Bone Thickness as well as patterns of facial growth. Alveolar Bone Thickness were very thin in high-angle participants on the labial and lingual aspects in the class III subgroup. The mandibular bone morphology were thinner in hyperdivergent subjects in class III malocclusion than class II hyperdivergent subjects.
In contrast to our study Hoang et al.[20] reported thicker alveolus in the anterior part of the jaw at the level of the alveolar crest and the tip of the root, in hyperdivergent subjects. Ponraj et al.[21] reported that subjects with horizontal facial types have thicker alveolus thus allowing the clinician to move lower incisors freely without fear of any adverse effect.
The present study thereby concludes that subjects with skeletal Class III malocclusion and hyperdivergent growth patterns should be dealt with extreme caution during fixed orthodontic treatment. Decreased bone density and cortical bone thickness on both the labial and lingual sides complicate the biomechanics. Extreme care should be taken to ensure that the mandibular incisor root remains inside the cancellous bone to achieve optimum orthodontic tooth movement.
Conclusion
Labial & Lingual bone density of mandibular symphysis in subjects having Skeletal Class III malocclusion were found to be maximum in hypodivergent facial type, whereas Lingual bone density were found to be minimum in the Hyperdivergent subjects. Labial bone density were reported to be the least among the Normodivergent subjects.
Labial & Lingual cortical plate thickness of the mandibular symphysis in subjects with skeletal Class III malocclusion were found to be maximum in Normo-divergent facial type followed by Hypo-divergent and minimum with Hyper-divergent facial type.
While treating cases of skeletal Class III malocclusion with fixed orthodontic appliances care should be taken in subjects with Hyper-divergent facial type since reduced bone density and cortical plate thickness may result in fenestration and dehiscence of roots in the mandibular anterior region.
Modifications should be done during bracket placement to ensure keeping the roots of mandibular incisors within the cancellous bone while treating cases of skeletal Class III malocclusion with Hyperdivergent or Vertical Facial type.
Further investigations and studies are required using a larger number of samples to validate the results of the present study.
Source of Funding
None.
Conflict of Interest
None.
References
- Wennström JL. Mucogingival considerations in orthodontic treatment. Semin Orthod. 1996;2(1):46-54. [Google Scholar]
- Lee S, Hwang S, Jang W, Choi YJ, Chung CJ, Kim KH. Assessment of lower incisor alveolar bone width using cone-beam computed tomography images in skeletal Class III adults of different vertical patterns. Korean J Orthod. 2018;48(6):349-56. [Google Scholar]
- Jiang N, Guo W, Chen M, Zheng Y, Zhou J, Kim SG. Periodontal ligament and alveolar bone in health and adaptation: Tooth Movement. Front Oral Biol. 2016;18:1-8. [Google Scholar]
- Wainwright WM. Faciolingual tooth movement: its influence on the root and cortical plate. Am J Orthod. 1973;64(3):278-302. [Google Scholar]
- Edwards JG. A study of the anterior portion of the palate as it relates to orthodontic therapy. Am J Orthod. 1976;69(3):249-73. [Google Scholar]
- Mulie RM, Hoeve AT. The limitations of tooth movement within the symphysis, studied with laminagraphy and standardized occlusal films. J Clin Orthod. 1976;10(12):882-93. [Google Scholar]
- Sassouni V. The Class II syndrome: differential diagnosis and treatment. Angle Orthod. 1970;40(4):334-75. [Google Scholar]
- Karlsen A. Craniofacial growth differences between low and high MP-SN angle males: a longitudinal study. Angle Orthod. 1995;65(5):341-50. [Google Scholar]
- Isaacson JR, Isaacson RJ, Speidel TM, Worms FW. Extreme variation in vertical facial growth and associated variation in skeletal and dental relations. Angle Orthod. 1971;41(3):219-248. [Google Scholar]
- Esenlik E, Sabuncuoglu F. Alveolar and symphysis regions of patients with skeletal class II division 1 anomalies with different vertical growth patterns. Eur J Dent. 2012;6(2):123-55. [Google Scholar]
- Ricketts R. Cephalometric synthesis. Am J Orthod. 1960;46(9):647-73. [Google Scholar]
- Bjork A. Prediction of mandibular rotation. Am J Orthod. 1969;55(6):585-99. [Google Scholar]
- Moshfeghi M, Nouri M, Mirbeigi S, Baghban A. Correlation between symphyseal morphology and mandibular growth. Dent Res J. 2014;11(3):375-79. [Google Scholar]
- Gousman J, Park J, Chae J. Evaluating mandibular symphysis bone density according to various skeletal patterns with CBCT. Orthod Craniofac Res. 2021;24(1):70-7. [Google Scholar]
- Kiliaridis S. The importance of masticatory muscle function in dentofacial growth. Semin Orthod. 2006;12(2):110-29. [Google Scholar]
- Gaffuri F, Cossellu G, Maspero C, Lanteri V, Ugolini A, Rasperini G. Correlation between facial growth patterns and cortical bone thickness assessed with cone-beam computed tomography in young adult untreated patients. Saudi Dent J. 2021;33(3):161-7. [Google Scholar]
- Kuitert R, Beckmann S, Van Loenen M, Tuinzing B, Zentner A. Dentoalveolar compensation in subjects with vertical skeletal dysplasia. Am J Orthod Dentofacial Orthop. 2006;129(5):649-57. [Google Scholar]
- Sadek M, Sabet N, Hassan I. Three-dimensional mapping of cortical bone thickness in subjects with different vertical facial dimensions. Prog Orthod. 2016;17(1). [Google Scholar]
- Silviana N. Alveolar Bone Thickness around Anterior Teeth in Different Classifications of Malocclusion: A Systematic Review. Insisiva Dent J Majalah Kedokteran Gigi Insisiva. 2022;11(1):41-53. [Google Scholar]
- Hoang N, Nelson G, Hatcher D, Oberoi S. Evaluation of mandibular anterior alveolus in different skeletal patterns. Prog Orthod. 2016;17(1):1-8. [Google Scholar]
- Ponraj R, Korath V, Vijayalakshmi D, Parameswaran R, Raman P, Sunitha C. Relationship of anterior alveolar dimensions with mandibular divergence in Class I malocclusion-A cephalometric study. J Clin Diagn Res. 2016;10(5):29-33. [Google Scholar]