- Visibility 650 Views
- Downloads 55 Downloads
- Permissions
- DOI 10.18231/j.jco.2025.005
-
CrossMark

Comparative evaluation of sequential maxillary molar distalization utilizing clear aligners in combination with micro-implants and Class II elastics for reinforcing the anchorage- A finite element model study
Abstract
Objectives: This study aims to perform a comparative evaluation of sequential maxillary molar distalization using clear aligners in combination with micro-implants and Class II elastics for reinforcing anchorage. The goal is to assess the biomechanical effectiveness and outcomes of these methods in achieving distalization without unwanted tooth movements.
Materials and Methods: A finite element model (FEM) study was conducted using the CBCT data of a 21-year-old female patient with Class II malocclusion. The 3D model of the maxilla and maxillary dentition was created and meshed for simulation. Five sub-models were developed to represent different treatment scenarios: clear aligners alone (control), aligners with Class II elastics using buttons or precision cuts, and aligners with micro-implants combined with elastics. Each model simulated sequential molar distalization with static loading forces. Displacement and stress responses were analyzed to determine the effectiveness and control of tooth movements.
Results: The FEM simulations revealed that the use of clear aligners with Class II elastics and micro-implants enhanced molar distalization efficiency while minimizing mesial displacement of anchorage teeth. Models with precision cuts and micro-implants showed superior anchorage control, reducing unwanted tipping and rotation. The greatest displacement was observed in models using precision cuts with Class II elastics, while the least displacement occurred in the control models.
Conclusion: The study concluded that Class II elastics provide superior control over molar movement compared to micro-implants when used with clear aligners for sequential maxillary molar distalization. Precision cuts on aligners offer better anchorage reinforcement than buttons.
Introduction
In recent years, Clear aligner treatment (CAT) has gained popularity for its aesthetic appeal and comfort. Advances in biomechanics and materials science have significantly improved the therapeutic efficacy of CAT, leading to its widespread acceptance among patients. Studies have shown that Invisalign aligners achieve an average accuracy of 50% in treatment outcomes.[1], [2]
Upper-molar distalization is a standard non-extraction approach for treating Class II malocclusion. It creates space, establishes Class I molar relationships, and achieves a normal overjet.[3]
Traditional methods, such as the distal jet and pendulum, often result in undesirable tooth movements during distalization, including, molar extrusion distal tipping, and proclination of anterior teeth due to anchorage loss.[4] CAT offers a solution for improved vertical dimension control, making it a more suitable option for patients with hyperdivergent or open bites.[5] It has been found that upper molar distalization through CAT has a high predictability rate of 88% for movements of 1.5 mm or more.[1] Nonetheless, molar distalization can result in anchorage loss due to reciprocal forces on anterior teeth, potentially causing alveolar defects in patients with thin cortical plates.[6], [7] Therefore, anchorage reinforcement is essential when using CAT for molar distalization.[8]
Class II intermaxillary elastics are frequently used in traditional fixed orthodontic treatment to strengthen anchorage along with maxillary molar distalization. However, recent studies suggest that Class II elastics may have more adverse effects than intended benefits, such as occlusal plane rotation and mandibular movement, leading to less aesthetic smiles.[9] Clear aligners, when combined with Class II elastics, may mitigate these issues by avoiding unwanted vertical movements due to the coverage of the entire dentition.[10] Ravera et al. conducted a study that showed the effectiveness of clear aligners using composite attachments along with Class II elastics in moving the upper first molars backward without causing noticeable tipping or vertical shifts.[11]
Micro-implant anchorage (MIA) has emerged as a reliable skeletal anchorage option for molar distalization, providing anchorage stability and reducing treatment time. As a temporary anchorage device (TAD), MIA offers biomechanical adaptability and less invasiveness, improving the predictability of clear aligner treatments.[12] However, there is limited research on the method of traction techniques for elastics coupled to micro-implants and clear aligners, leaving a gap in clinical recommendations for orthodontists on how to combine these approaches effectively.[13]
The computational technique known as the FEM makes it possible to quantitatively characterize the initial movement of teeth following force loading. In biomechanical research, this technique is frequently employed to analyse displacement and stress responses in a range of settings. The usefulness of FEM in modelling tooth displacement patterns in orthodontics has been shown in recent studies.[14] Nevertheless, prior models have either been restricted to just one tooth or have only examined the sagittal/horizontal plane, neglecting to take consecutive molar distalization into account.[15]
This article delves into a comprehensive comparative evaluation of sequential maxillary molar distalization techniques. Specifically, it juxtaposes the utilization of clear aligners with Class II elastics versus micro-implants as anchorage reinforcement. Through the lens of finite element modelling, we explore the biomechanical intricacies underlying each approach, shedding light on their respective advantages, limitations, and overall efficacy.
Materials and Methods
A 21-year-old female patient with a class II malocclusion, a full dentition without third molars provided the cone-beam computed tomography (CBCT) data. The CBCT results were acquired for medical use. The Ethics Committee accepted the use of the participant's CBCT data after she gave signed, informed consent for the conduct of the study. 360° of centered rotation was used for the full field of view (FoV) CBCT scan. 100 kV of voltage and current at 4 mA of current were used, and the exposure period was 15 s. A total of 668 horizontal CBCT slices were rebuilt, with each slice's thickness fixed at 0.15 mm.
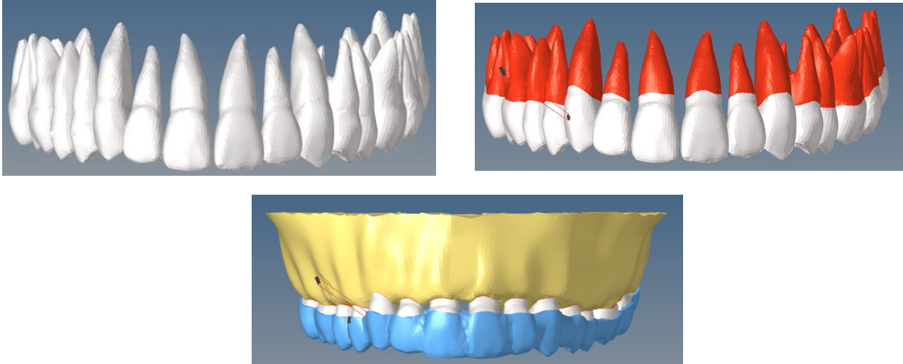
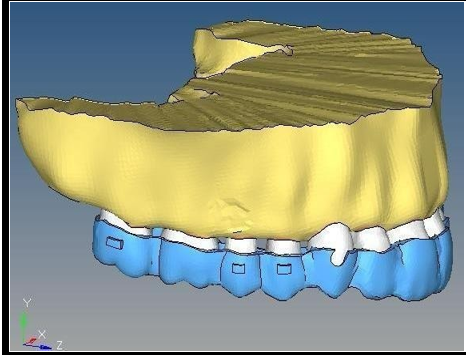
In order to finalize the meshing of the entire 3D model, Hyper mesh 2019 was implemented as a pre-processor. The exterior surface of the tooth roots was expanded by 0.25 mm to restore the PDL as a homogeneous layer. After being offset by 1.3 mm, the maxilla bone moved inward to set up a model of the cancellous bone. The cancellous bone was subsequently removed from the maxilla bone, resulting in the formation of the cortical bone. For retention purposes, vertical rectangular attachments (2 × 3 × 1 mm) were affixed to the buccal surfaces of all premolars, while the upper 2nd molars were equipped with horizontal rectangular attachments (3 × 2 × 1 mm). The tooth crowns and attachments were extended by 0.5 mm to resemble a CA appliance. Two micro-implants, each measuring 1.5 mm x 8 mm, were placed between the second premolars and first molar at a height of 5 mm from the alveolar crest and an inclination of 60 degrees with respect to the occlusal plane.[16], [17]
Creating sub-models from the original 3D model
A 3D FE-based model was created by importing the original model along with the appliances. Using SolidWorks software, three-dimensional geometric surface models of the upper jaw and upper teeth were created using digital data of the upper jaw and upper teeth.
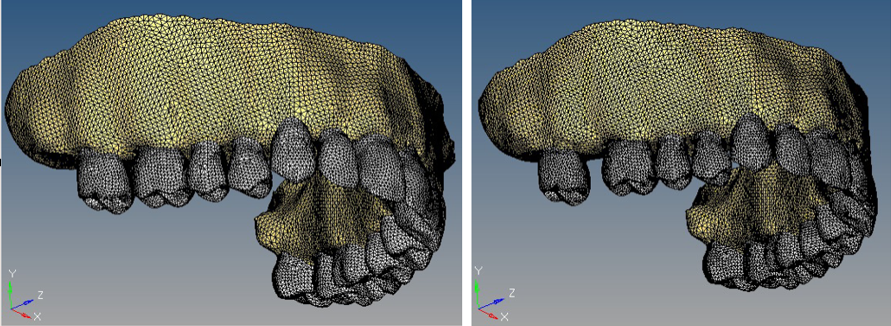
The resultant step File were then imported to HyperMesh software to enable 3D meshing of teeth and maxilla using tetrahedral mesh type. In [Figure 1], the meshing of the Maxilla bone with teeth and a clear aligner model is illustrated, employing tetrahedral elements. The Maxilla bone is meshed using 0.7 mm tetrahedral elements, with each individual tooth connected by a mesh of 0.5 mm of the same element type, as depicted in [Figure 2]. This configuration represents the realistic scenario of the connection between bone and teeth or the attachment of tissues represented by the Periodontal Ligament, using a triangular shell mesh of 0.5 mm element size with thickness of 0.2 mm ([Figure 3]). Additionally, displays the geometric mesh of the clear aligner made of Class II elastic material, utilizing a 0.5 mm tetrahedral mesh. Three-dimensional ten-node tetrahedral structural solid, was utilized. The material properties like Young's modulus (or modulus of elasticity) and the Poisson ratio ([Table 1]) were assigned to all the components.[18], [19], [20], [21]
Five sub-models were divided into two group sets in order to replicate the streamlined sequential molar distalization procedure. The second molars in group set I moved 0.2 mm distal, while the first molars in group set II moved 0.2 mm distal after the second molars had been set in a target position.
Each set has five sub-sets:
(Control Group): Maxilla and maxillary dentition with Clear Aligners.
(Exp Group): A with Class II elastics worn over the aligner from mandibular first molar to the button on the labial surface of the canine.
(Exp Group): A with Class II elastics worn over the aligner from mandibular first molar to the precision cut present on the canine region of aligner.
(Exp Group): A with one mini-screw in the inter-radicular region of first molar and second premolar. Elastic will be worn over the aligner from mini- screw to the buttons on labial surface of canines.
(Exp Group): A with one mini-screws between the inter-radicular region of first molar and second premolar. Elastics will be worn on each side over the aligner from mini-screw to precision cut present on the canine region of the aligner.
Models C (C1 & C2) and E (E1 & E2) were featured with precision cuts. Aligners at the labial surface of the canines were incorporated with a hook known as Precision cut. Models B (B1 and B2) and D (D1 & D2) had buttons (height: 1 mm and diameter: 3 mm) on the upper canines, with cut out in the corresponding sections of the CA. The button's interface and the tooth surface were fused together. Clinical research and practical applications were considered while designing the precision cuts and buttons.[13]
|
Material/Properties |
Modulus of Elasticity (MPa) |
Poisson’s Ratio |
|
Bone |
13700 |
0.3 |
|
Periodontal Ligament |
0.67 |
0.45 |
|
Teeth |
19600 |
0.3 |
|
Aligner |
528 |
0.36 |
The boundary and contact conditions of the sub; models
Regarding the boundary specifications, the maxilla and temporal bones were restricted to the full range of motion of the nodes in their superior region. Bonding contacts were formed at the interfaces of, cortical bone-PDL, spongious-cortical bone, bone-micro-implants, teeth, PDL, tooth buttons, and attachment. Movement between the contact surfaces is impeded by this bonding. Furthermore, it was anticipated that the connections between neighbouring teeth were not separated from their interfaces.
Loading method
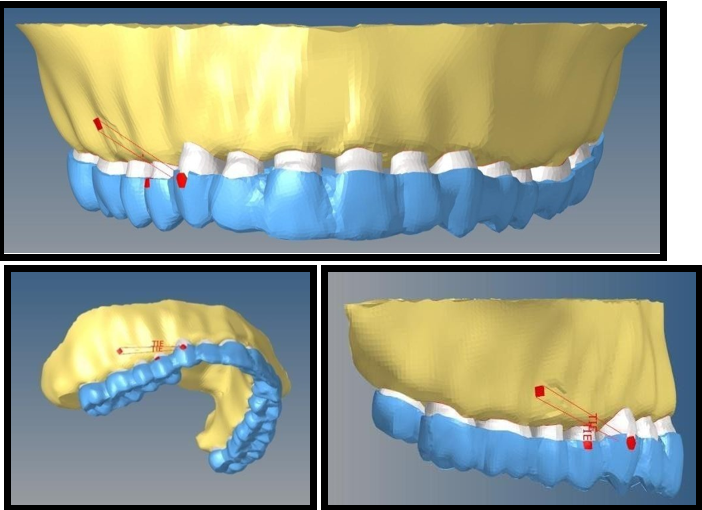
In the FEM simulation, static loading was implemented. The step distance for molar distalization was determined to be 0.2 mm. In group set I, the second molar was moved distally by 0.2 mm to establish a loaded condition CA. Subsequently, the mismatch between the CA and the original dentition was employed to apply the loading force. In group set II, the second molar was moved distally by 0.2 mm, followed by the first molar, which moved distally by 0.2 mm to produce a active clear aligner. Lastly, a spring connected to the micro-implants and the buttons or precision incisions on each side applied a force of 120 g in models B and D.
NiTi springs are used to simulate the application of elastic traction. Preliminary experiments were conducted to investigate the force generated by Class II elastics, that was simulated by delivering a force of 120 g through a spring in models C and E.
Coordinate systems and outcomes
Meshing is the process of discretizing elements into finite elements, a crucial step aimed at achieving output that corresponds to real-world results. The accuracy and reliability of Finite Element Analysis (FEA) predictions heavily depend on the quality of the mesh, making careful consideration of meshing parameters essential for meaningful and applicable outcomes. The discretization technique separated the FE mesh. [Table 2] shows the nodes and linear elements for each sub-model. For comparison, two coordinate systems were defined20.The global coordinate system was developed for the entire dentition, with the vertical plane represented by the y-axis (+ superior, −inferior), the coronal plane represented by the x-axis (+ left, −right), and the sagittal plane represented by the z-axis (+ posterior, −anterior). The local coordination system was designed for individual tooth as follows: the y-axis (+lingual, −buccal), the x-axis (+mesial, −distal), and the z-axis (+apical, −crown). We calculated the displacement pattern of both complete dentition and individual teeth.
Palatal root apex and mesio-buccal cusp served as the reference points for posterior teeth, whereas tooth cusp and root apex served as the same for anterior teeth.
The summary of the nodes and elements for the bone, teeth, and clear aligner is presented in[Table 2].
|
|
A1 |
A2 |
B1 |
B2 |
C1 |
C2 |
D1 |
D2 |
E1 |
E2 |
|
Nodes |
92546 |
92674 |
92546 |
92674 |
92546 |
92674 |
92546 |
92674 |
92546 |
92674 |
|
Elements |
507880 |
506628 |
507880 |
506628 |
507880 |
506628 |
507880 |
506628 |
507880 |
506628 |
Results
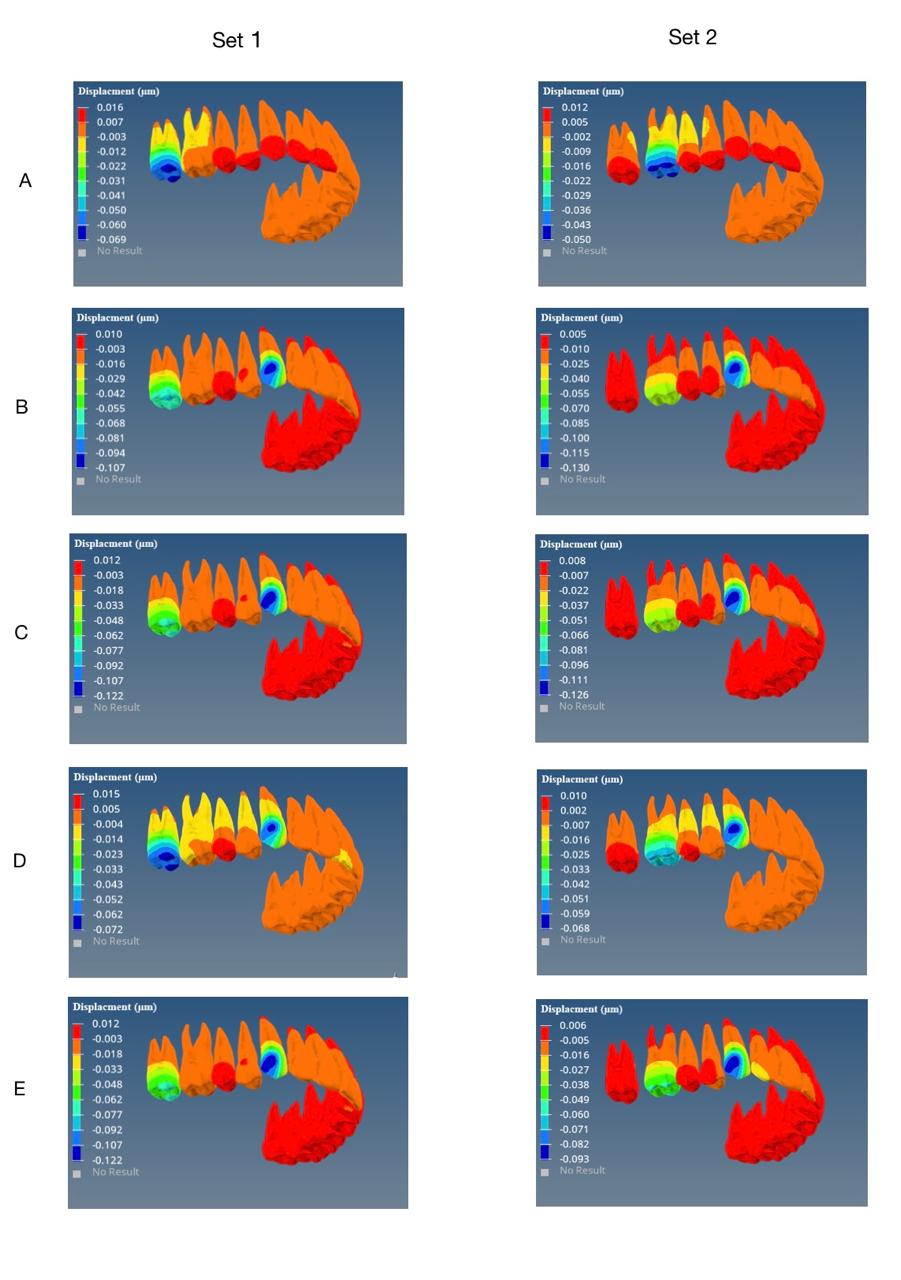
The major direction of displacement for the posterior teeth was mesio-distal direction. The second molars in group set I had a distobuccal tipping tendency and were shifted distally. The premolars and first molars moved mesially with a mesio-buccal tipping tendency as a result of the reciprocal forces caused by CA. The first molar in group II migrated distally and had a disto-buccal tilting tendency. In every model, the anchorage teeth and the distally migrated molars moved in opposing directions due to the reciprocal force. The clear aligner applied reciprocal force to the second molars and other anchorage teeth during the distal movement of first molar.
The displacement for all the sub-sets are summarized in [Figure 5], [Figure 6].
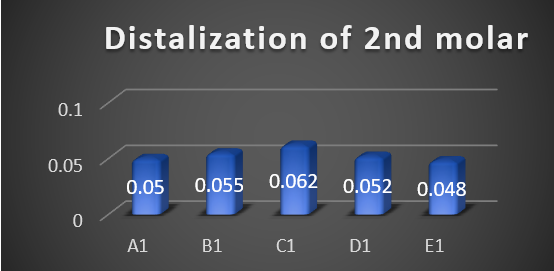
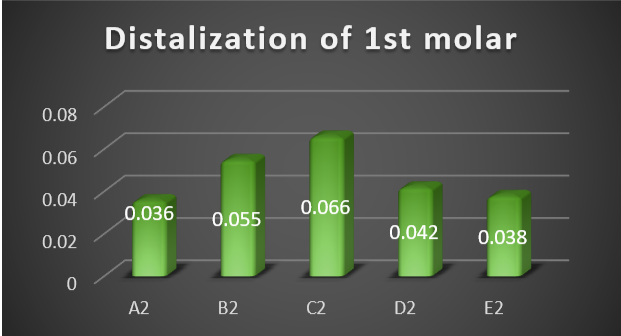
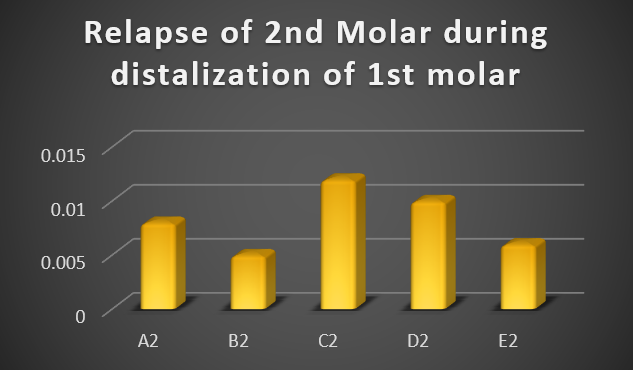
Model C1 (0.062 um) had the greatest probability for total displacement for 2nd molar and model C2 (0.066 um) for 1st molars. This was achieved by attaching class II elastics to the aligner by precision cuts, and 120 gms traction force. On the contrary, the least displacement probablity was with model A1 (0.005 um) for 2nd molar and A2 (0.036 um) for 1st molar which was without any anchorage reinforcement. The mesial displacement of 2nd molar during distalization of 1st molar in Set1 due to the reciprocal forces was most in model A(0.11) and the least in model D(0.005).
The anteriors exhibited an intrusion and mesiolabial tipping tendency in all models due to the reciprocal force. The axis of rotation was located near the midpoint of the root's middle third. The unwanted movement of the anteriors was diminished in models C1 and E1 in comparison to the movement observed in the other models of set 1. Model D had the lowest degree of labial tipping in set 2, with model E following closely behind.
The most amount of labial tipping was seen in model A as no anchorage reinforcement was given.
Discussion
Clear aligner therapy (CAT) has distinct advantages for molar distalization, including enhanced aesthetics, patient comfort, and superior vertical control. However, the lack of auxiliaries other than composite attachments during the treatment can lead to varying degrees of proclination of the anteriors due to the reciprocal forces from molar distalization. This can result in anchorage loss, a common challenge during the use of CAT for molar distalization.[22]
Class II intermaxillary elastics are commonly used in fixed orthodontic treatment to reinforce anchorage in treating Class II malocclusion. Despite their effectiveness, the combination of intermaxillary elastics with clear aligners remains underexplored. The existing clinical literature is mostly composed of retrospective studies and case reports, lacking in-depth evaluation of this treatment approach.[23]
Additionally, the use of micro-implants in conjunction with clear aligners requires further exploration, as there is no established method for handling larger distalization distances (greater than 3 mm). These challenges underscore the need for more precise guidance and research on the combination of micro-implants and CAT. [24]
We found that the distalizing molars were distobuccally tipped as a result of the distalization force, whereas the anchorage teeth were mesiobuccally tipped as a result of the reciprocal force.
During the distalization of the second molar, the distal movement was responsible for 52.86% of the 0.25-mm step distance in the absence of anchoring reinforcement.
In contrast, tilting and rotation made up the remaining proportion, with the mesial movement of the first molars accounting for 26.18%. The reason for the increased effectiveness in distalization of the maxillary 1st molar compared to the maxillary 2nd molar may be explained by this.[25]
The current investigation showed that Aligners attached to micro-implants through precision cuts or Class II elastics through precision cut provided superior anchorage control and reinforcement. This method was more effective in distributing the anchorage force to the entire dentition. The utilization of Class II intermaxillary elastics connected to the lingual button on the canine exhibited the greatest reduction in the relapse potential of second molars. Safe force application ranges from 100 to 200 g were reported, with larger forces increasing the efficiency of molar distalization.[16] Park et al. also considered that a large magnitude of force, up to 200 g, was not excessive when used for the distal movement of molars.[26]
Nevertheless, it's crucial to acknowledge the limitations of this study. Firstly, we assumed uniform thickness of the periodontal ligament (PDL), However, in actuality, the PDL has a shape resembling an hourglass, with its narrowest point occurring at the mid-root level. [27] Moreover, the material properties of PDL have been a subject of historical controversy, with a range of 0.01 to 100 MPa for elastic modulus. While some scholars argue for the nonlinearity of its elastic modulus, research indicates that this nonlinearity primarily impacts stress magnitude rather than the actual movement pattern of teeth26. Secondly, this static examination solely offers an overview of the earliest inclinations towards movement. The clinical outcomes are significantly affected by cumulative effects of alternating forces and bone remodelling processes. Lastly, tooth movement is influenced by multiple biological factors, such as the close proximity of the root to the cortical bone, penetration or proximity of the sinus, shape of the root, and periodontal metabolism.[27] Therefore, it's crucial to exercise caution when translating these conclusions into clinical practice.
Conclusion
The comparative evaluation of sequential maxillary molar distalization using clear aligners, with Class II elastics and micro-implants as anchorage reinforcement, demonstrated significant insights into the effectiveness of these methods. The results of this finite element model study revealed that using Class II elastics as anchorage reinforcement achieved superior distalization of maxillary molars compared to micro-implants. Class II elastics provided better control over molar movement, minimizing unwanted tipping and extrusion, and ensuring more predictable outcomes.
Precision cutting exhibited enhanced anchoring control and decreased tooth displacement in comparison to the use of buttons for attaching elastics to aligners. The biomechanical advantages of Class II elastics, coupled with the aesthetic and comfort benefits of clear aligners, offer a compelling alternative to traditional orthodontic approaches. However, there was a small rise in unwanted molar tipping and rotation. These findings can improve decision-making processes for orthodontists, leading to optimized treatment strategies for patients requiring molar distalization.
Ethics Approval and Consent to Participate
Not applicable.
Consent for Publication
All the authors provide their consent for the publication.
Availability of Data and Material: All the required data is attached and sent along with the manuscript. If there is anything more required from the journal side, we are ready to provide them.
Competing Interests
Not applicable.
Source Funding
Self-funding.
Author's Contribution
All the authors have contributed extensively to the study. Author 1 contributed to the conception, design, and data acquisition. Author 2 contributed to the conception and interpretation of the data and drafted and critically revised the manuscript. Author 3 contributed to the statistical analysis of the data. Author 4 and Author 5 contributed to the conception, design, and revision of the manuscript.
References
- Rossini G, Parrini S, Castroforio T, Deregibus A, Debernardi C. Efficacy of clear aligners in controlling orthodontic tooth movement: a systematic review. Angle Orthod. 2015;85(5):881-90. [Google Scholar]
- Haouili N, Kravitz N, Vaid N, Ferguson D, Makki L. Has Invisalign improved? A prospective follow-up study on the efficacy of tooth movement with Invisalign. Am J Orthod Dentofac. 2020;158(3):420-5. [Google Scholar]
- Al-Thomali Y, Basha S, Mohamed R. Pendulum and modified pendulum appliances for maxillary molar distalization in class II malocclusion - a systematic review. Acta Odontol Scand. 2017;75(6):394-401. [Google Scholar]
- Simon M, Keilig L, Schwarze J, Jung B, Bourauel C. Treatment outcome and efficacy of an aligner technique-regarding incisor torque, premolar derotation and molar distalization. BMC Oral Health. 2014;14. [Google Scholar]
- Caruso S, Nota A, Ehsani S, Maddalone E, Ojima K, Tecco S. Impact of molar teeth distalization with clear aligners on occlusal vertical dimension: a retrospective study. BMC Oral Health. 2019;19(1). [Google Scholar]
- Patterson B, Foley P, Ueno H, Mason S, Schneider P, Kim K. Class II malocclusion correction with Invisalign: is it possible?. Am J Orthod Dentofac. 2021;159(1):41-9. [Google Scholar]
- Evangelista K, Vasconcelos K, Bumann A, Hirsch E, Nitka M, Silva M. Dehiscence and fenestration in patients with class I and class II division 1 malocclusion assessed with cone-beam computed tomography. Am J Orthod Dentofac. 2010;138(2):131-4. [Google Scholar]
- Xu Y, Xie J. Comparison of the effects of mini-implant and traditional anchorage on patients with maxillary dentoalveolar protrusion. Angle Orthod. 2017;87(2):320-7. [Google Scholar]
- Janson G, Sathler R, Fernandes TM, Branco NC, Freitas MR. Correction of class II malocclusion with class II elastics: a systematic review. Am J Orthod Dentofac. 2013;143(3):383-92. [Google Scholar]
- Staderini E, Ventura V, Meuli S, Maltagliati L�, Gallenzi P. Analysis of the changes in occlusal plane inclination in a class II deep bite "teen" patient treated with clear aligners: a case. Report Int J Env Res Pub He. 2022;19(2). [Google Scholar]
- Ravera S, Castroforio T, Garino F, Daher S, Cugliari G, Deregibus A. Maxillary molar distalization with aligners in adult patients: a multicenter retrospective study. Prog Orthod. 2016;17. [Google Scholar]
- Ma Q, Conley R, Wu T, Li H. Asymmetric molar distalization with miniscrews to correct a severe unilateral Class III malocclusion. Am J Orthod Dentofac. 2016;149(5):729-68. [Google Scholar]
- Bowman S, Celenza F, Sparaga J, Papadopoulos M, Ojima K, Lin J. Creative adjuncts for clear aligners, part 1: class II treatment. J Clin Orthod. 2015;49:83-94. [Google Scholar]
- Ayidaga C, Kamiloglu B. Effects of variable composite attachment shapes in controlling upper molar distalization with aligners: a nonlinear finite element study. J Healthcare Eng. 2021;2021(1):1-8. [Google Scholar]
- Rossini G, Schiafno M, Parrini S, Sedran A, Deregibus A, Castroforio T. Upper second molar distalization with clear aligners: a finite element study. Appl Sci. 2020;10(21). [Google Scholar]
- Ammoury M, Mustapha S, Dechow P, Ghafari J. Two distalization methods compared in a novel patient-specific finite element analysis. Am J Orthod Dentofac. 2019;156(3):326-62. [Google Scholar]
- Jasmine M, Yezdani A, Tajir F, Venu R. Analysis of stress in bone and microimplants during en-masse retraction of maxillary and mandibular anterior teeth with diferent insertion angulations: a 3-dimensional finite element analysis study. Am J Orthod Dentofac. 2012;141(1):71-80. [Google Scholar]
- Cheng Y, Gao J, Fang S, Wang W, Ma Y, JZ. Torque movement of the upper anterior teeth using a clear aligner in cases of extraction: a finite element study. Prog Orthod. 2022;23(1). [Google Scholar]
- Ma Y, Li S. The optimal orthodontic displacement of clear aligner for mild, moderate and severe periodontal conditions: an in vitro study in a periodontally compromised individual using the finite element model. BMC Oral Health. 2021;21(1). [Google Scholar]
- Gomez J, Pena F, Martinez V, Giraldo D, Cardona C. Initial force systems during bodily tooth movement with plastic aligners and composite attachments: a three-dimensional finite element analysis. Angle Orthod. 2015;85(3):454-60. [Google Scholar]
- Ammar H, Ngan P, Crout R, Mucino V, Mukdadi O. Three-dimensional modelling and finite element analysis in treatment planning for orthodontic tooth movement. Am J Orthod Dentofac. 2011;139(1):59-71. [Google Scholar]
- Saif B, Pan F, Mou Q, Han M, Bu W, Zhao J. Efficiency evaluation of maxillary molar distalization using Invisalign based on palatal rugae registration. Am J Orthod Dentofac. 2022;161(4):372-81. [Google Scholar]
- Dianiskova S, Rongo R, Buono R, Franchi L, Michelotti A, Anto D. Treatment of mild class II malocclusion in growing patients with clear aligners versus fixed multibracket therapy: a retrospective study. Orthod Craniofac Res. 2022;25(1):96-102. [Google Scholar]
- Auladell A, Iglesia F, Quevedo O, Walter A, Puigdollers A. The efficiency of molar distalization using clear aligners and mini-implants: two clinical cases. Int Orthod. 2022;20(1). [Google Scholar]
- Liu X, Wu J, Cheng Y, Gao J, Wen Y, Zhang Y. Efective contribution ratio of the molar during sequential distalization using clear aligners and micro-implant anchorage: a fnite element study. Prog Orthod. 2023;24(1). [Google Scholar]
- Park H, Lee S, Kwon O. Group distal movement of teeth using micro - screw implant anchorage. Angle Orthod. 2005;75(4):602-11. [Google Scholar]
- Tanne K, Sakuda M, Burstone C. Three-dimensional finite element analysis for stress in the periodontal tissue by orthodontic forces. Am J Orthod Dentofac. 1987;92(6):499-505. [Google Scholar]
- Abstract
- Introduction
- Materials and Methods
- Creating sub-models from the original 3D model
- The boundary and contact conditions of the sub; models
- Loading method
- Coordinate systems and outcomes
- Results
- Discussion
- Conclusion
- Ethics Approval and Consent to Participate
- Consent for Publication
- Competing Interests
- Source Funding
- Author's Contribution
- References