- Visibility 26 Views
- Downloads 10 Downloads
- DOI 10.18231/j.jco.2022.013
-
CrossMark

Transverse digital dental analysis of patients treated with self ligating Damon Q system with different patterns of retention- A longitudinal study with three years follow up
Introduction
The chief objective of orthodontics is to achieve an esthetic, functional and stable arch form. An accurate diagnosis and framing of treatment planning is the definitive key to a successful treatment, which incorporates both the active and retention phase of the treatment. The arch form and arch dimensions have a significant impact while diagnosing any case since it gives information about the position in which the teeth can be moved,[1] followed by finalizing a treatment plan. They influence the esthetics and stability of the dentition. Every malocclusion is secured by balanced muscular forces, especially in the mandibular canine and first molar region.[2] Arch width increases during alignment in extraction and non-extraction cases. Most changes occur in the premolar area, then in the canine region, followed by the molar region.[3] However, pure dental expansion is unacceptable due to alveolar limitations, except in the cases with mild crowding and those requiring a buccal tipping effect.[4] In 1925, Lundstorm focused on the need to examine the apical base to govern the occlusion. According to his study, the normal occlusion gained by mechanical treatment is not always followed by the development of the apical base in conjugation with the position of the teeth, which ultimately results in the replase of the occlusion attained.[5] Little, did a study on 65 cases treated with first premolar extraction using conventional brackets and reported an increment of 1mm of mandibular inter-canine distance during treatment in 60% of cases. However, it is constricted by 2mm in 60 of the 65 cases.[6] This result was also supported by studies performed by Uhde,[7] Walter[8] and Heiser.[9] Furthermore, in Damon bracket system expansion of the buccal segments can be achieved by producing broader arch forms.[10] The low friction Damon brackets produces more expansion in the posterior region, with fewer changes in the inter canine width.[10], [11] Several studies show that the inter canine, inter premolar and inter molar width increase with Damon bracket system, in non-extraction cases.[12], [13], [14], [15] Further, a few studies performed with first premolar extraction cases states that inter canine width increased but the intermolar width reduced when treated with Damon bracket system.[16]
The literature is unclear about the stability of the changes achieved after treatment with Damon bracket system. Therefore, the present study not only evaluates the mean transverse widths of the maxillary and mandibular canines, premolar and molars but also evaluates the changes after treatment and after 3 years of follow-up, in cases treated with all four first premolar extraction. This study also compares the changes occurring in the patients who were under complete retention for three years and those who were under retention for two years and discontinued retention for the next consecutive year.
Material and Methods
A longitudinal study was approved by the Institutional Ethics Committee (TMDCRC/IEC/18-19). The sample size was calculated using the nMaster 2.0 software. The power of the study was taken to be 80% and the Confidence Interval (C.I.) of 95%.[17] Minimum sample size for each group was estimated to be 20. Written consent was obtained from all the patients selected for the study.
Inclusion criteria
The post pubertal patients with permanent dentition, age 15-18 years,
No missing or supernumerary teeth,
No previous history of orthodontic treatment, with class I molar relation bilaterally with moderate to severe proclination, ANB 0° to 4°, crowding 8-10 mm in the upper and lower arch,
Treated with all four first premolar extractions, with Damon Q bracket system were selected
The patients with cleft lip and palate, tooth out of arch and patients requiring expansion or contraction of the arches were excluded.
The cases selected were the ones treated with all four first premolar extraction. Damon Q brackets were bonded with banding in the first and second molars. Further, the leveling and alignment were initiated on 0.014” Cu NiTi wire. Following alignment, the anterior segment of both the arches was consolidated. Eventually, the retraction was commenced on 0.019” x 0.025” SS wire. The archwires were coordinated according to the original arch form of the patient. Retraction was done from the molar tube’s hook to the crimpable hooks (Libral Traders) fixed between the lateral incisors and canine. Following the retraction, final settling was done and a stable occlusion was obtained. Fixed retainers were given from canine to canine in both the arches (Orthoclassic stranded retention wire- .0195 inch, Mc Minnville, Oregon). The average treatment time for all the cases was 30-36 months.
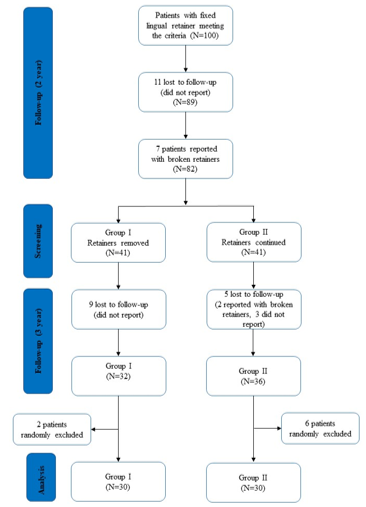
100 patients falling in our inclusion criteria were selected. Their pretreatment and post-treatment study models were collected from the department. These patients were recalled every six months for check till 2 years of completion of their treatment. 89 out of 100 patients reported after 2 years. The examination of these 89 patients showed that 7 patients had partially broken retainers, whereas, 82 patients had intact retainers without any damage. The retainers were removed from both the arches of 41 patients. The patients with retainers were instructed to maintain oral hygiene, and avoid hard and sticky food to prevent breakage of the retainers. All these 82 patients were recalled also after 1 year. 32 out of 41 patients with no retainers reported for the second follow-up, whereas, 36 out of 41 patients who previously had intact retainers reported, but 2 of them were excluded due to partially broken retainers. Further, 30 from 32 (without retainers) and 30 from 34 patients (with retainers) were selected randomly with a lottery system. Therefore, we had two groups, group I (GI) with two years retention and group II (GII) with 3 years retention. The follow-up records were taken and models were poured for both the groups. The study design is shown in ([Figure 1]).
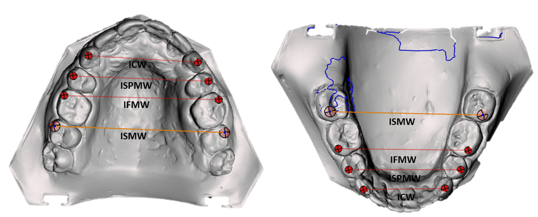
The models were scanned using an intraoral scanner (3 Shape TRIOS 3 Digital Impression Solution). The intercanine width from cusp tips of the canines, the inter premolar width from buccal cusp tips, inter molar width from mesio-buccal cusp tips were measured using third-party software (Auto Desk Mesh Mixer) ([Figure 2]). The measurements were done again after 4 weeks by the same observer. Further, the parameters among the groups were compared.
Statistical Analysis
All statistical analysis were done using Statistical Product and Service Solutions (SPSS) Statistics for Windows, Version 21.0. Armonk, NY: IBM Corporation. The level of significance was at 5% (0.05), P value less than 0.05 was considered to be statistically significant, and the power of the study was set at 80%. The mean and standard deviation for the continuous data was calculated for both the groups. Kolmogorov–Smirnov test of normality was done to assess the distribution of the data and it was found that the data were normally distributed (P >0.05). The operator’s calibration was validated by using the intra-class correlation coefficient (ICC) which was 0.93. Repeated measures Analysis of Variance with Bonferroni post hoc test was done to compare the parameters at different time intervals. The mean difference in post-treatment and retention periods (T1–T2) was compared between GI and GII by independent t-test (Unpaired t-test).
Result
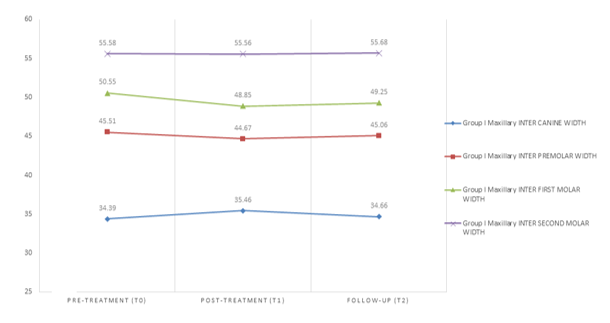
The study comprised 16 males and 14 females in group I and 12 males and 18 females in group II. The mean age was 16.52 years in GI and 16.55 years in GII ([Table 1]). The mean value of GI showed that the maxillary inter canine width was 34.39 mm at T0 which increased to 35.46 mm at T1 but reduced to 34.66 mm at T2. A similar pattern of changes was seen in inter premolar and inter first molar width.
|
|
Group |
Total |
|||
|
GI |
G II |
||||
|
Total |
N |
30 |
30 |
60 |
|
|
% |
100.0% |
100.0% |
100.0% |
||
|
Gender |
Male |
N |
16 |
12 |
28 |
|
% |
53.3% |
40.0% |
46.6% |
||
|
Female |
N |
14 |
18 |
32 |
|
|
% |
46.6% |
60.0% |
53.3% |
||
|
Age (years) |
Mean |
16.52 (.99) |
16.55 (.93) |
- |
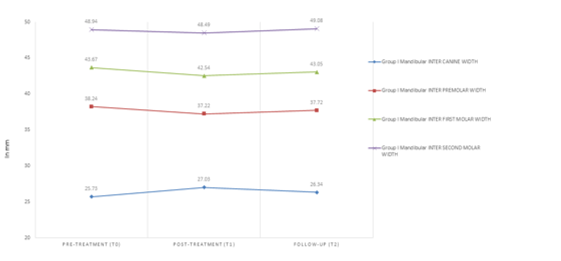
However, the inter second molar width remained unchanged with negligible variation ([Table 2], [Figure 3]). Further, in the mandibular parameters, the average inter canine width was 25.73 mm which increased to 27.03 mm after treatment but decreased to 26.34 mm. The inter premolar reduced from 38.24mm to 37.22mm after treatment but showed a slight increase after follow-up, from 37.22 mm to 37.72 mm. The pattern of variation for inter first molar width from T0 to T1 and from T1 to T2 was the same as inter premolar width. The inter second molar width remained almost unchanged after treatment but increased at follow up ([Table 2], [Figure 4]). Most of the parameters changed after treatment but depicted the tendency to return to their original value.
|
|
GI |
|||||||
|
|
Maxillary |
Mandibular |
||||||
|
|
ICW (mm) |
ISPMW (mm) |
IFMW (mm) |
ISMW (mm) |
ICW (mm) |
ISPMW (mm) |
IFMW (mm) |
ISMW (mm) |
|
T0 |
34.39 |
45.51 |
50.55 |
55.58 |
25.73 |
38.24 |
43.67 |
48.94 |
|
T1 |
35.46 |
44.67 |
48.85 |
55.56 |
27.03 |
37.22 |
42.54 |
48.49 |
|
T2 |
34.66 |
45.06 |
49.25 |
55.68 |
26.34 |
37.72 |
43.05 |
49.08 |
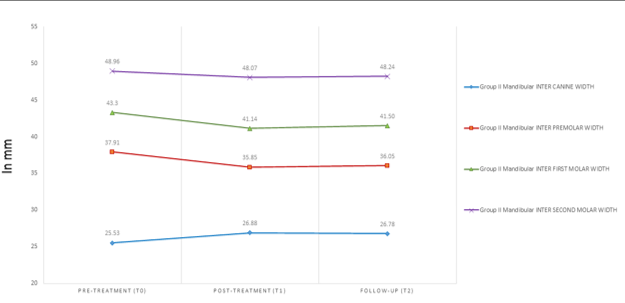
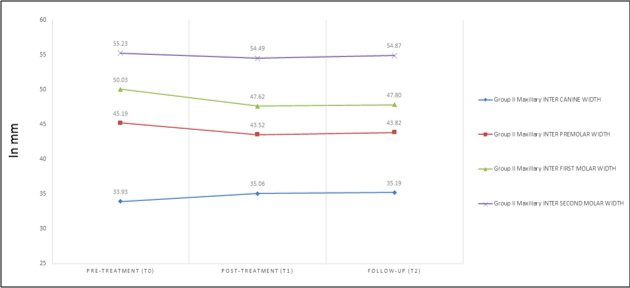
The parameters GII showed that the maxillary inter canine, inter premolar and molars width, changed from T0 to T1 but presented negligible variation from T1 to T2 ([Table 3], [Figure 6]).
Similarly, the mandibular inter canine and inter premolar width slightly changed at follow-up. Inter second molar width remained equivalent at all the stages but inter first molar width reduced from T0 to T1 but increased at T2 ([Table 3], [Figure 5]).
|
|
GII |
|||||||
|
|
Maxillary |
Mandibular |
||||||
|
|
ICW (mm) |
ISPMW (mm) |
IFMW (mm) |
ISMW (mm) |
ICW (mm) |
ISPMW (mm) |
IFMW (mm) |
ISMW (mm) |
|
T0 |
33.93 |
45.19 |
50.03 |
55.23 |
25.53 |
37.91 |
43.30 |
48.96 |
|
T1 |
35.06 |
43.52 |
47.62 |
54.49 |
26.88 |
35.85 |
41.14 |
48.07 |
|
T2 |
35.19 |
43.82 |
47.80 |
54.87 |
26.78 |
36.05 |
41.50 |
48.24 |
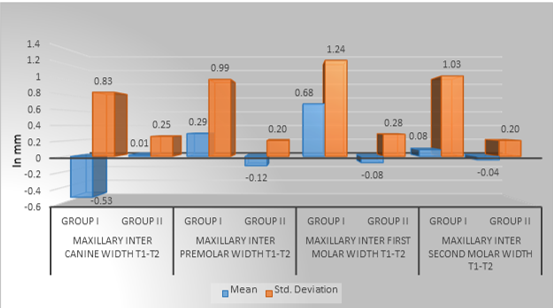
The maxillary intergroup difference of the mean of the parameters between T1 and T2 resulted that the mean difference being significant for inter canine and inter first molar width. However, the inter premolar and inter second molar width showed an insignificant mean difference ([Table 4], [Figure 7]).
|
|
Mean(mm) |
Standard deviation (mm) |
Mean Difference (mm) |
t |
P value |
|
|
Max ICW (T1-T2) |
GI |
-.53 |
.83 |
-.55 |
-2.57 |
.018* |
|
GII |
.01 |
.25 |
||||
|
Max ISPMW (T1-T2) |
GI |
.29 |
.99 |
.41 |
1.89 |
.072 |
|
GII |
-.12 |
.20 |
||||
|
Max IFMW (T1-T2) |
GI |
.68 |
1.24 |
.76 |
2.88 |
.009* |
|
GII |
-.08 |
.28 |
||||
|
Max ISMW (T1-T2) |
GI |
.08 |
1.03 |
.13 |
.53 |
.596 |
|
GII |
-.04 |
.20 |
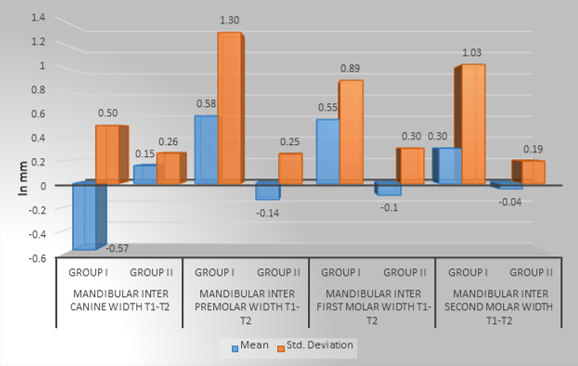
The mandibular intergroup difference of the mean of the parameters between T1 and T2 presented that the mean difference was significant for all the parameters except inter second molar width ([Table 5], [Figure 8]).
|
|
|
Mean (mm) |
Standard Deviation (mm) |
Mean Difference (mm) |
t |
P value |
|
Man ICW (T1-T2) |
GI |
-.57 |
.50 |
-.72727 |
-5.299 |
.000* |
|
GII |
.15 |
.26 |
|
|
|
|
|
Man ISPMW (T1-T2) |
GI |
.58 |
1.30 |
.72727 |
2.548 |
.019* |
|
GII |
-.14 |
.25 |
||||
|
Man IFMW (T1-T2) |
GI |
.55 |
.89 |
.65455 |
3.063 |
.006* |
|
GII |
-.10 |
.30 |
||||
|
Man ISMW (T1-T2) |
GI |
.30 |
1.03 |
.35000 |
1.515 |
.145 |
|
GII |
-.04 |
.19 |
While comparing the maxillary & mandibular parameters at different time intervals in GI showed that the variation of mandibular inter canine width was significant. Further, the Bonferroni post hoc test revealed a significant difference between the measurements at T0 and T1 ([Table 6]).
|
GI |
T0 |
T1 |
T2 |
F |
P-value |
|
|
ICW (mm) |
Maxillary |
34.39 |
35.46 |
34.66 |
1.32 |
.273 |
|
Mandibular |
25.73a |
27.03b |
26.34 |
3.50 |
.035* |
|
|
ISPMW (mm) |
Maxillary |
45.51 |
44.67 |
45.06 |
.83 |
.439 |
|
Mandibular |
38.24 |
37.22 |
37.72 |
.74 |
.477 |
|
|
IFMW (mm) |
Maxillary |
50.55 |
48.85 |
49.25 |
2.11 |
.127 |
|
Mandibular |
43.67 |
42.54 |
43.05 |
1.21 |
.302 |
|
|
ISMW (mm) |
Maxillary |
55.58 |
55.56 |
55.68 |
.02 |
.978 |
|
Mandibular |
48.94 |
48.49 |
49.08 |
.34 |
.707 |
The comparison of the maxillary & mandibular parameters at different time intervals in GII showed the difference of the maxillary inter premolar, inter first molar width and mandibular inter canine, inter premolar and inter first molar width were significant. Further, these significant differences in all the parameters were due to the changes observed at T0-T1 and T0-T2, except, maxillary inter premolar width which was only because of T0-T1 ([Table 7]).
|
GII |
T0 |
T1 |
T2 |
F |
P-value |
|
|
ICW (mm) |
Maxillary |
33.93 |
35.06 |
35.19 |
2.28 |
.108 |
|
Mandibular |
25.53a |
26.88b |
26.78b |
4.81 |
.011* |
|
|
ISPMW (mm) |
Maxillary |
45.19a |
43.52b |
43.82 |
4.66 |
.012* |
|
Mandibular |
37.91a |
35.85b |
36.05b |
5.67 |
.005* |
|
|
IFMW (mm) |
Maxillary |
50.03a |
47.62b |
47.80b |
6.24 |
.003* |
|
Mandibular |
43.30a |
41.14b |
41.50b |
5.94 |
.004* |
|
|
ISMW (mm) |
Maxillary |
55.23 |
54.49 |
54.87 |
1.10 |
.337 |
|
Mandibular |
48.96 |
48.07 |
48.24 |
1.17 |
.314 |
Discussion
The measurement of the arch width at the anterior and posterior segments of the upper and lower arch holds importance.[5] According to Reed and Moorees;[18] White and Barrow;[19] Deckock and Sillman,[20] the increase in the arch width might be seen till the eruption of permanent canines, mainly in the anterior segment. However, it decreases in both the regions, once the eruption is complete.
The intercanine width is defined differently by various authors. For instance, De la Cruz et al, defined this as the distance between the cusp tips of both canines on either side.[21] Heiser et al, describe intercanine width as the distance between canine cusp tips or estimated cusp tips in the attrited tooth surfaces in maxillary and mandibular arches.[9] While, Paulino et al, stated the intercanine distance as a linear distance between the cusps of canine or in cases of evident wearing, the distance between the centers of the worn out surfaces.[22]
The average intercanine width in the primary dentition is approximately 25.2 mm in the mandibular arch and 28.8 mm in the maxillary arch, whereas, for permanent dentition, it is 24 mm and 31 mm in the mandible and maxilla respectively.[23] The intermolar dimension is measured from the distance between the mesiobuccal cusp tips of contralateral molars in the arch. Howe et al reported an average maxillary intermolar width to be 37.4 mm for males and 36.2 mm for females.[24] Shapiro,[24] McCauley,[25] Steiner[26] and Strang[2] reported that the lower inter-molar and inter-canine width showed relapse in the post retention period, therefore, needs to be considered unchanged.
Several factors are responsible for relapse after orthodontic treatment. The most considerable reason for relapse is the change in the original arch form.[25] Further, the lower inter canine and intermolar width is said to be an apt indicator of an individual’s muscular balance, which directs the limits for arch expansion.[27] Corey Shook,[28] conducted a study to compare the changes in maxillary arch width and buccal corridor, in the patients treated with Damon and Conventional brackets. The research was done using the pictures of the patients. The study concluded that intercanine and intermolar width increases after treatment in both the groups but there was no significant difference between the groups. However, our study shows that the intercanine width increases but the intermolar width decreases in both GI and GII after treatment. Further, Jacob Lima,[12] performed a study comparing changes in dental arch dimensions in cases treated with conventional and Damon systems. The study states that the maxillary inter canine, inter first and second premolar and intermolar widths increased significantly in cases treated with the Damon system. Further, the mandibular intercanine and first premolar width increased significantly. However, inter second premolar and intermolar width increases insignificantly. On the contrary, our study shows an increase in intercanine width but a reduction in inter premolar and intermolars width in both GI and GII after treatment. Atik,[13] performed a study using radiographs and maxillary dental models of the patients treated with a non-extraction line of treatment, to compare Damon 3MX bracket system and conventional bracket system. They concluded that the intercanine, inter first and second premolar and intermolar width increases significantly with Damon bracket system. However, this study substantiates our study with respect to increase of intercanine width but varies in respect to inter premolar and intermolar width, as the posterior width reduces in our study. Fleming,[14] Liliana[4] and Pandis,[15] reported that the intercanine, interpremolar and intermolar widths increase in patients treated with a non-extraction line of treatment with Damon bracket system. Scott,[16] performed research in which the mandibular arch widths were measured in the patients treated with first premolars extraction using Damon 3 bracket system. This reported that the lower intercanine width increased whereas, the intermolar width reduced after treatment. This study supports our study, as the intercanine width was increased and intermolar width was reduced after treatment in both the arches and in both the groups (GI and GII). After observing the changes in all the previous studies with Damon bracket system[12], [13], [14], [15], [16] and our study, this might state that, the anterior width increases but the posterior width decreases in patients treated with first premolars extraction. Further, according to our study, the changes remain stable if the patient is kept under complete retention but anterior, as well as posterior arch width, tends to return to the original position when the retainers are removed. Our study was limited to a young adult group; future research should include a larger age range. We have also concentrated on the Demon bracket system; but, in the future, it should also emphasize other bracket systems.
Conclusion
The intercanine width increased, whereas, inter premolar and inter molars width reduced after treatment in cases treated with all four first premolar extraction using the Damon Q bracket system.
The cases which were under retention for two years showed reduction in intercanine width and increase in premolar and molars arch width at follow-up. However, the difference was insignificant.
The cases which were under retention for three years, showed negligible changes in inter canine, inter premolar and inter molars width at follow-up.
The changes achieved after treatment tends to revert to the original dimensions after removal of retainers.
This could be concluded that, the original arch widths should be maintained during treatment, else, relapse might occur after removal of the retainers.
Source of Funding
None.
Conflict of Interest
None.
References
- B Podesser, S Williams, H P Bantleon, H Imhof. Quantitation of transverse maxillary dimensions using computed tomography: a methodological and reproducibility study. Eur J Orthod 2004. [Google Scholar]
- R H W. The fallacy of denture expansion as a treatment procedure. Angle Orthod 1949. [Google Scholar]
- P M Cattaneo, M Treccani, K Carlsson. Transversal maxillary dento-alveolar changes in patients treated with active and passive self-ligating brackets: A randomized clinical trial using CBCT-scans and digital models. Orthod Craniofac Res 2011. [Google Scholar]
- L A Maltagliati, Y I Myiahira, L Fattori, C Filho, L Cardoso. Transversal changes in dental arches from non-extraction treatment with self ligating brackets. Dental Press J Orthod 2013. [Google Scholar]
- Ai L. Malocclusion of the teeth regarded as a problem in connection with the apical base. Int J Orthod 1925. [Google Scholar]
- R M Little, T R Wallen, R A Riedel. Stability and relapse of mandibular anterior alignment- first premolar extraction cases treated by traditional edgewise orthodontics. Am J Orthod 1981. [Google Scholar]
- M D Uhde, C Sadowsky, E A Begole. Long-term stability of dental relationships after orthodontic treatment. Angle Orthod 1983. [Google Scholar]
- D C Walter. Comparative changes in mandibular canine and first molar widths. Angle Orthod 1962. [Google Scholar]
- W Heiser, M Richter, A Niederwanger, N Neunteufel, S Kulmer. Association of the canine guidance angle with maxillary and mandibular intercanine widths and anterior alignmentrelapse: Extraction vs nonextraction treatment. Am J Orthod Dentofac Orthop 2008. [Google Scholar]
- . Damon System: The Workbook. Orange, Calif: Ormco. 2004. [Google Scholar]
- D H Damon. The rationale, evolution and clinical application of the self-ligating bracket. Clin Orthod Res 1998. [Google Scholar]
- N Lima, C Fr Falcão Ic De, M De Freitas, K V De Lima, D Valarelli, F P Cançado, R H. Comparison of Changes in Dental Arch Dimensions in Cases Treated with Conventional Appliances and Self-Ligating Damon System. Open Dent J 2018. [Google Scholar]
- Atik Ezgi, Cigersemra. An assessment of conventional and self-ligating brackets in Class I maxillary constriction patients. Angle Orthod 2014. [Google Scholar]
- P S Fleming, R T Lee, V Marinho, A Johal. Comparison of maxillary arch dimensional changes with passive and active self-ligation and conventional brackets in the permanent dentition: A multicenter, randomized controlled trial. Am J Orthod Dentofac Orthop 2013. [Google Scholar]
- N Pandis, A Polychronopoulou, T Eliades. Self-ligating vs conventional brackets in the treatment of mandibular crowding: A prospective clinical trial of treatment duration and dental effects. Am J Orthod Dentofac Orthop 2007. [Google Scholar]
- P Scott, A T Dibiase, M Sherriff, M T Cobourne. Alignment efficiency of Damon3 self- ligating and conventional orthodontic bracket systems: A randomized clinical trial. Am J Orthod Dentofac Orthop 2008. [Google Scholar]
- M R De Almeida, R R A Pedrin, R R De Almeida, C F-Mir. A Prospective Clinical Trial of Arch Width Changes Evaluated through Dental Casts in Consecutively Treated Non-extraction and Extraction Cases. Dentistry 2011. [Google Scholar]
- C F Moorrees, R B Reed. Biometrics of crowding and spacing of the teeth in the mandible. Am J Phys Anthropol 1954. [Google Scholar]
- A Barrow, J White. Developmental changes of the maxillary and mandibular dental arches. Angle Orthod 1952. [Google Scholar]
- J H Sillman. Dimensional changes of the dental arches: Longitudinal study from birth to 25 years. Am J Orthod 1964. [Google Scholar]
- C A De La, P Sampson, R M Little, J Artun, P A Shapiro. Long-term changes in arch form after orthodontic treatment and retention. Am J Orthod Dentofac Orthop 1995. [Google Scholar]
- V Paulino, V Paredes, J L Gandia, R Cibrian. Prediction of arch length based on intercanine width. Eur J Orthod 2008. [Google Scholar]
- R T Lee. Arch width and form: a review. Am J Orthod Dentofac Orthop 1999. [Google Scholar]
- P A Shapiro. Mandibular dental arch form and dimension. Am J Orthod 1974. [Google Scholar]
- D R Mccauley. The cuspid and its function in retention. Am J Orthod Oral Surg 1944. [Google Scholar]
- C Steiner. Orientation of the teeth in dental arches. Angle Orthod 1934. [Google Scholar]
- N Sharma, A Miglani, M Nanda, N Sonawane, S A Abraham. Importance of retention and relapse in orthodontics- a review. TMU J Dent 2019. [Google Scholar]
- C Shook, S M Kim, J Burnheimer. Maxillary arch width and buccal corridor changes with Damon and conventional brackets: A retrospective analysis. Angle Orthod 2016. [Google Scholar]