- Visibility 170 Views
- Downloads 29 Downloads
- DOI 10.18231/j.jco.2023.005
-
CrossMark

Evaluation of reliability & reproducibility of cephalometric measurements obtained from computerised software (CS8100SC) compared with manual tracing
- Author Details:
-
 Prakhar Pragya *
Prakhar Pragya *
-
Sankalp Sood
-
Monika Mahajan
-
Dimple Chainta
-
KS Negi
Introduction
Broadbent[1] and Hofrath[2] introduced cephalometry in 1931 which is an indispensible tool used in diagnosis and treatment of dental and skeletal malocclusions. Conventionally, manual tracing is considered as benchmark in cephalometric analysis.[3] Early 1990s witnessed advancement in digital radiography with the transfer of landmarks on conventional radiographs to video monitors using digitized pads[4], [5] and more direct and indirect forms of digitization were available, such as charged couple device[6] (CCD) and storage phosphor plates[7] respectively. These reduced radiation exposures,[8], [9] but direct digitization of radiographs was found to be more reproducible and accurate than indirect digitization.[10] In digital images, landmarks can either be marked manually or by automated computerized identification,[3] however automated computerized identification of cephalometric landmarks does not compete with manual identification in terms of accuracy of landmark position.[3], [4], [5], [6], [7], [8], [9], [10], [11]
Both manual and digital cephalometrics have their own advantages and disadvantages. Manual tracing is tiresome, time taking and associated with human errors like inaccurate landmark identification, measurement and calculation problems.[12] Digital imaging offers several advantages over manual tracing by reducing the time needed for data acquisition and analysis.[13] These are also easy to store and multiple analysis can be done over a very short period of time but has the disadvantages of both projection and tracing errors.[14] Interpretation of the various types of errors are necessary in cephalometric analysis to reach correct conclusion. Both Reliability [15], [16] and Reproducibility[15], [16] are crucial in the investigations for determining errors in measurement.
CS8100SC imaging software is a recently introduced cephalometric software. We did not come across any study in the literature that shows its reliability and reproducibility. So, the purpose of our study was to compare and assess the reliability and reproducibility of cehalometric measurements with digital computerized software in comparison to manual tracing.
Materials and Methods
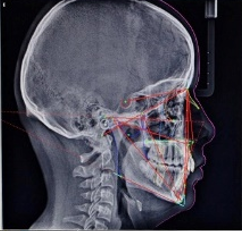
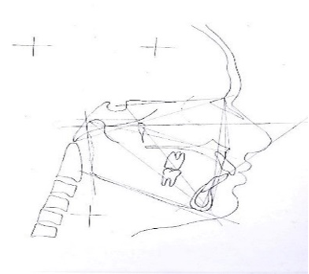
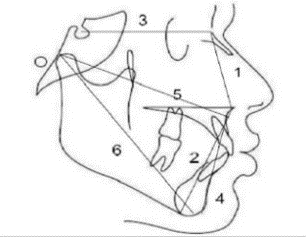
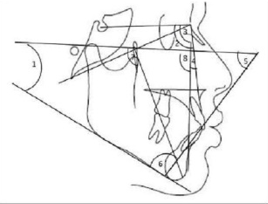
Institutional review board approval was obtained from Ethical committee of Govt. Dental College and Hospital, Shimla, Himachal Pradesh, India with letter approval noHFW(GDC)B(12)44/2009-6097. We enrolled 50 orthodontic patients in the age group 15-30 years having Angle’s class I malocclusion undergoing treatment in the Department of Orthodontics and Dentofacial Orthopedics at H. P Govt. Dental College and Hospital, Shimla, Himachal Pradesh, India For Digital tracing, lateral cephalogram of the subjects were taken in the Natural Head Position with seated condyle. Standardized 8” ×10” dry view laser imaging film was used for each subject. All cephalograms were linked to the computer with Windows 10 operating system. The image was saved and then transferred into CS8100SC Imaging software ([Figure 1]). The dentofacial relationships and landmarks was identified using tool from CS8100SC toolbar after calibration of the image on a 1:1 scale. To assist landmark identification wherever necessary, the images were zoomed, enhanced for contrast and adapted for auto grey levels whereas for Manual tracing, hard copy of digital image was taken with the help of Dry View 5700 laser image printer and landmarks were identified manually ([Figure 2]) on acetate tracing paper 0.36mm using 4H pencil on an X-ray view box. Tracing was done by same operator to minimize error. The digital and manual tracing were then compared to evaluate differences in any of the measurements. 5 cephalograms were analyzed daily to avoid the human fatigue errors. To determine reproducibility,10 randomly selected cephalograms were retraced manually and digitally after 7 weeks of interval. Out of the 14 Parameters selected for the study 6 were linear ([Figure 3]) and 8 were angular ([Figure 4]). A total of 700 readings were recorded from the 50 patients who were enrolled in the study. Statistical significance was set at P value<0.05. Mean and standard deviations were calculated for all the data. Paired t- test was used to evaluate statistical significance for comparing mean values between corresponding data sets. Intraclass correlation coefficients (ICC) was used to determine in reliability as well as to evaluate reproducibility for each cephalometric parameter. ICC value of 0.75 was indicative of low agreement whereas ICC values of >0.75 indicated of a good agreement. All continuous variables were calculated as Mean ± SD ([Table 1]).
Results
The manual and digital cephalometric readings were compared ([Table 1]) and no statistical differences were found for ANS-Me, Co-Pt. A, Co-Gn, Facial axis, FMIA and IMPA whereas significant differences were found for N-ANS, A-Pog, S-N, FMA, SNA, SNB, ANB and Facial angle. Intraclass correlation coefficient value for Reliability ([Table 2]) showed high agreement for all the parameters except ANB. Intraclass correlation coefficient values for Reproducibility ([Table 3]) showed high agreement for all the parameters except Facial axis, Facial angle, ANB and FMIA which showed less reproducibility.
|
Parameters |
Digital |
Manual |
p value |
||
|
Mean |
SD |
Mean |
SD |
||
|
N-ANS (mm) |
49.41 |
2.81 |
49.88 |
2.88 |
0.000** |
|
ANS- Me(mm) |
60.89 |
5.30 |
60.86 |
5.30 |
0.790 |
|
A- Pog (mm) |
49.52 |
4.62 |
49.92 |
4.57 |
0.002** |
|
S-N (mm) |
65.72 |
3.66 |
66.02 |
3.55 |
0.008** |
|
Co-Pt. A(mm) |
82.49 |
4.75 |
82.28 |
4.80 |
0.159 |
|
Co-Gn (mm) |
108.42 |
6.90 |
108.20 |
6.55 |
0.171 |
|
FMA (degree) |
23.68 |
4.92 |
24.10 |
4.91 |
0.023* |
|
SNA (degree) |
82.62 |
3.36 |
81.80 |
3.27 |
0.000** |
|
SNB (degree) |
79.56 |
3.18 |
78.98 |
3.12 |
0.000** |
|
ANB (degree) |
3.04 |
0.89 |
2.84 |
0.76 |
0.023* |
|
Facial Axis (degree) |
90.54 |
3.24 |
90.20 |
2.83 |
0.183 |
|
Facial Angle (degree) |
88.90 |
2.40 |
88.22 |
2.21 |
0.000** |
|
FMIA (degree) |
60.30 |
5.00 |
61.02 |
6.75 |
0.215 |
|
IMPA (degree) |
95.46 |
5.78 |
94.62 |
7.52 |
0.167 |
|
N-ANS (mm) |
49.41 |
2.81 |
49.88 |
2.88 |
0.000** |
|
Parameters |
ICC |
CI |
|
N-ANS (mm) |
0.962 |
0.846-0.990 |
|
ANS-Me (mm) |
0.972 |
0.886-0.993 |
|
A-Pog (mm) |
0.974 |
0.894-0.993 |
|
S-N (mm) |
0.996 |
0.983-0.999 |
|
Co-Pt. A (mm) |
0.976 |
0.902-0.994 |
|
Co-Gn (mm) |
0.979 |
0.916-0.995 |
|
FMA (degree) |
0.939 |
0.753-0.985 |
|
SNA (degree) |
0.952 |
0.806-0.988 |
|
SNB (degree) |
0.946 |
0.784-0.987 |
|
ANB (degree) |
-0.531 |
-5.163-0.620 |
|
Facial axis (degree) |
0.964 |
0.855-0.991 |
|
Facial angle (degree) |
0.872 |
0.486-0.968 |
|
FMIA (degree) |
0.955 |
0.820-0.989 |
|
IMPA(degree) |
0.979 |
0.914-0.995 |
|
Parameters |
1st reading ICC |
2nd reading ICC |
|
N-ANS (mm) |
0.960 |
0.981 |
|
ANS-Me (mm) |
0.948 |
0.956 |
|
A-Pog (mm) |
0.974 |
0.966 |
|
S-N (mm) |
0.995 |
0.991 |
|
Co-Pt.A (mm) |
0.962 |
0.984 |
|
Co-Gn (mm) |
0.984 |
0.961 |
|
FMA (degree) |
0.973 |
0.952 |
|
SNA (degree) |
0.960 |
0.959 |
|
SNB (degree) |
0.956 |
0.967 |
|
ANB (degree) |
0.621 |
0.633 |
|
Facial axis (degree) |
0.760 |
0.924 |
|
Facial angle (degree) |
0.946 |
0.787 |
|
FMIA (degree) |
0.700 |
0.760 |
|
IMPA (degree) |
0.856 |
0.891 |
Discussion
This study was done to compare 14 commonly used cephalometric parameters obtained from digital tracing followed by hand tracing to check the reliability and reproducibility. Inaccuracy in landmark identification is a major source of error in cephalometric analysis and it is greatly affected by operator experience. For digital method mouse-driven cursor was used to identify the landmarks and the measurements were determined automatically whereas in manual tracing landmarks identification and measurements were both done manually. According to Gravely and Benzies et al.[17] when the landmarks are traced manually on digital radiographs it results in less measurement errors, so it may be the best strategy.
In our study we found that there was no statistically significant difference in 6 parameters (ANS-Me, CO-Pt. A, Co-Gn, Facial axis, FMIA and IMPA) thereby implying that there is no difference in readings between manual and digital tracings and CS8100SC software was found to be acceptable for recording the values of these parameters. Similar non-significant findings were reported by Shahakbari et al.[18] for the value of ANS-Me, Mahto et al.[3] for Co-Pt. A, Ganna et al.[19] for Co-Gn, Cavdar et al.[20]for facial axis, Farooq et al.[21] for FMIA and Gregston et al.[5] for IMPA. However contrary to our findings regarding these six parameters, Izgi et al.[22] found significant value for ANS-Me, Co-Pt.A, Co-Gn and found that problem in landmark identification was the reason behind this. Similarly, Ganna et al.[19] found significant value for FMIA, IMPA and found problem in identifying lower incisor apex due to superimposition of structures and FH plane. Remaining 8 parameters (N-ANS, A-Pog, S-N, FMA, SNA, SNB, ANB and Facial angle) were statistically significant in our study. These parameters came significant because of difficulty in identification of landmarks. During manual tracing different reference planes were constructed to assist in identifying points such as Gn and Go which were not possible with on screen digitization. Regarding N-ANS, we found difficulty in identification of point N similar to the finding reported by Sekiguchi and Savara et al.[23] who also found difficulty in marking point N due to inaccurate visualization of nasofrontal suture. In our study A-Pog was also found significant due to problem in identification of point A and Pog and Prabhakar et al.[24] also found difficulty in identification of point A in their studies. S-N was found to be significant due to difficulty in locating point N and similar finding was reported by Agrawal et al.[25] but contrary finding was reported by Albarkati et al.[15] We also observed FMA value to be significant due to difficulty in locating point Gonion because of poorly defined anatomical outline, a double image and localization away from the mid-sagittal plane. Similar finding was reported by Santoro et al.[26] whereas contrary to this, Mahto et al.[3] did not find this to be significant. The values of SNA, SNB and ANB was found significant due to problem in identification of point nasion and point A. Albarkati et al.[15] and Gregston et al.[5] have also reported significant value of SNA and SNB. Contrary to this finding Ganna et al.,[19] Mahto et al.[3] and Khan et al.[27] found non-significant value of SNA and SNB. Santoro et al.[26] also found significant value of ANB due to difficulty in identification of landmarks like point A and nasion but contrary to this, Izgi et al.[22] and Mahto et al.[3] found non-significant value of ANB. Facial angle was also found significant in our study due to difficulty in locating Nasion, Pog and FH plane, similar findings were reported by Baumrind et al.[12] and Santoro et al.[26] for facial angle. Contrary to this, Agrawal et al.[25] found non significant value of facial angle. In our study we found good reliability of all the parameters except for ANB ([Table 2]). Previous studies by Santoro et al.[26] also found trouble in identification of point A. Sekiguchi and Savara et al.[23] found nasion to be difficult to identify when the nasofrontal suture is not accurately visualized. These findings support the less reliability of ANB, whereas Facial axis, Facial angle ANB and FMIA showed less reproducibility in comparison to other parameters investigated in this study ([Table 3]). According to Chen et al.[11] porion, orbitale and gonion shows great variation and thus demonstrates low level of reproducibility. According to Santoro et al.,[26] point A is notorious for its poor reproducibility. The values of Facial axis, Facial angle, ANB showed less reproducibility in our study probably because landmarks like point A, Porion, Orbitale having poor reproducibility were included in them. In our study the measurement difference was less than 2 units ([Table 1]) and according to Schultze et al.[28] when the measurement difference is less than 2 units (mm or degree) that is within the one standard deviation of norm values of conventional cephalometric analysis between the two techniques, it is considered to be clinically insignificant or clinically acceptable.
Conclusion
Digital tracing using CS8100SC Imaging software significantly correlates with traditional manual tracing technique for 8 out of 14 parameters. No statistical differences were found for ANS-Me, Co-Pt. A, Co-Gn, FMIA, Facial axis and IMPA. Whereas significant differences were found for N-ANS, S-N, A-Pog, FMA, SNA, SNB, ANB and Facial angle but were clinically acceptable. Digital measurements obtained from software CS8100SC are reliable except for the ANB which showed low agreement. Whereas Reproducibility between manual and digital tracing is good except for ANB, Facial axis, Facial angle and FMIA. Hence, it is concluded that CS8100SC software can be used for the cephalometric measurements of the parameters included in the study.
Source of Funding
None.
Conflict of Interest
There is no conflict of interest in our study.
References
- BH Broadbent. A new x-ray technique and its application to orthodontia. Angle Orthod 1931. [Google Scholar]
- H Hofrath. The importance of X-ray distance and distance imaging for the diagnosis of jaw aneomalis. Progress Orthod 1931. [Google Scholar]
- RK Mahto, OP Kharbanda, R Duggal. A comparison of cephalometric measurements obtained from two computerized cephalometric softwares with manual tracing. J Indian Orthod Soc 2016. [Google Scholar]
- DB Forsyth, WC Shaw, S Richmond. Digital imaging of cephalometric radiography. Part I: Advantages and limitation of digital imaging. Angle Orthod 1996. [Google Scholar]
- MD Gregston, T Kula, P Hardman, A Glaros, K Kula. Comparison of conventional and digital radiographic methods and cephalometric analysis software: I. Hard tissue. Semin Orthod 2004. [Google Scholar]
- WS Boyle, GE Smith. Charge couple semiconductor devices. Bell Syst Tech J 1970. [Google Scholar]
- HV Seggern. Photostimulable x-ray storage phosphorus. A review of the present understanding. Brazilian J Phys 1999. [Google Scholar]
- H Visser. Dose reduction by direct digital cephalometrics radiography. Angle Orthod 2001. [Google Scholar]
- K Seki, T Okano. Exposure reduction in cephalography with a digital photostimulable phosphor imaging system. Dentomaxillofac Radiol 1993. [Google Scholar]
- A Richardson. Comparison of traditional and computerised method of cephalometric analysis. Eur J Orthod 1981. [Google Scholar]
- YJ Chen, SK Chen, HF Chang, KC Chen. Comparison of landmark identification in traditional versus computer- aided digital cephalometry. Angle Orthod 2000. [Google Scholar]
- S Baumrind, RC Frantz. The reliability of head film measurements 2. Conventional angular and linear measures. Am J Orthod 1971. [Google Scholar]
- M Erkan, HG Gurel, M Nur, B Demirel. Reliability of four different computerized cephalometric analysis programs. Eur J Orthod 2012. [Google Scholar]
- JF Gravely, PM Benzies. The clinical significance of tracing error in cephalometry. Brit J Orthod 1974. [Google Scholar]
- SF Albarakati, KS Kula, AA Ghoneima. The reliability and reproducibility of cephalometric measurements a comparison of conventional and digital method. Dentomaxillofac Radiol 2012. [Google Scholar]
- G Power, J Breckon, M Sherriff, F Mcdonald. Dolphin Imaging Software: Analysis of the accuracy of cephalometric digitization and orthognathic prediction. Int J Oral Maxillofac Surg 2005. [Google Scholar]
- JF Gravely, PM Benzies. The clinical significance of tracing error in cephalometry. Brit J Orthod 1984. [Google Scholar]
- R Shahakbari, M Pahlevankashi, M Eshghpour, A Ataii. Comparison of Digital Cephalometric Tracing by Onyx Ceph Software versus Manual Method. Int J Contemp Dent Med Rev 2018. [Google Scholar]
- PS Ganna, SK Shetty, MK Yethadka, A Ansari. An Evaluation of the errors in cehalometric measurement on scanned lateral cephalometric measurement on scanned lateral cephalometric images using computerised cephalometric program and conventional tracing. J Ind Orthod Soc 2014. [Google Scholar]
- K Cavdar, S Ciger, A Zeynep. A comparison of conventional and computerised cephalometric methods. Clin Dent Res 2011. [Google Scholar]
- MU Farooq, MA Khan, S Imran, A Sameera, A Qureshi, SA Ahmed. Assessing the reliability digitalized cephalometric analysis in comparison with manual cephalometric analysis. J Clin Diagn Res 2016. [Google Scholar]
- E Izgi, FN Pekiner. Comparative Evaluation of Conventional and Onyx Ceph Dental Software Measurements on Cephalometric Radiography. Turk J Orthod 2019. [Google Scholar]
- T Sekiguchi, BS Savara. Variability of cephalometric landmarks used for face growth studies. Am J Orthod 1972. [Google Scholar]
- R Prabhakar, P Rajakumar, MK Karthikeyan, R Saravanan, NR Vikram, A Reddy. A hard tissue cephalometric comparative study between hand tracing and computerized tracing. J Pharm Bioall Sci 2014. [Google Scholar]
- N Agarwal, DK Bagga, P Sharma. A Comparative study of Cephalometric Measurements with Digital versus Manual Methods. J Ind Orthod Soc 2011. [Google Scholar]
- M Santoro, K Jarjoura, J Thomas. Accuracy of digital and analogue cephalometric measurements assessed with sandwich technique. Am J Orthod Dentofac Orthop 2006. [Google Scholar]
- FA Khan, P Joneja, DS Choudhary, R Ahmed, S Tikekar. Differentiation of evaluation of reliability of cephalometric analysis of cephalometrically diagnosed skeletal class I malocclusion using available digital imaging software such as IMAGE J and ICY and traditional manual tracing. Indian J Dent Sci 2021. [Google Scholar]
- R Schultze, M Dent, MB Gloede, GM Doll. Landmark identification on direct digital versus film based cephalometric radiographs- A human skull study. Am J Orthod Dentofac Orthop 2002. [Google Scholar]