- Visibility 58 Views
- Downloads 7 Downloads
- DOI 10.18231/j.jco.2023.023
-
CrossMark

Management of Class III malocclusion by orthodontic clockwise rotation of maxillo-mandibular complex – A case report
- Author Details:
-
Amulya Sundararaj
-
 G. Sreejith Kumar *
G. Sreejith Kumar *
-
Babukuttan Pillai
-
Dan Thomas
Introduction
Class III malocclusions are the least frequent sagittal malocclusions with greatest prevalence among Asian ethnic groups.[1] Younger and adult patients presented with a combination of skeletal, dentoalveolar and functional issues and most often, management of this malocclusion is complicated by problems in vertical and transverse dimensions. Compromised facial aesthetics and functions are the main reasons why these patients seek orthodontic treatment.[2] Skeletal Class III malocclusions are the most challenging problems to treat particularly due to the unfavourable growth pattern of mandible and associated dental compensations.[3] Many of these cases require orthopaedic correction in growing children and orthognathic surgery in non-growing patients for the best treatment outcome. In adults, though orthognathic surgery is often the ideal treatment, many patients refuse to take surgery due to the cost-benefit considerations and invasive nature of the procedure.[4] But in borderline skeletal problems, orthodontic camouflage may be considered to attain acceptable occlusion, improved aesthetics and optimum function.[5] The main objective of orthodontic camouflage involves proclination of the maxillary anteriors and retroclination of the mandibular anteriors by selective extractions, fixed appliance with class III intermaxillary elastics and en masse distalization of mandibular dentition using temporary anchorage devices.[6]
In Skeletal Class III cases, treatment planning by conventional surgical method includes advancement or setback of maxilla and/or mandible along the occlusal plane.[5] But in Class III patients with vertical problems, like hypo or hyperdivergent faces, this procedure may resulted in compromised facial esthetics. In such situations, sagittal movement of jaws along with rotation of Maxillo-Mandibular complex (MMc) or alteration of the occlusal plane improves facial balance and esthetics.[7], [8] Based on this concept, Eric Liou has proposed a strategy of orthodontic clockwise rotation of MMc or ‘orthognathic camouflage’ for patients with mild to moderate Class III malocclusions and hypodivergent faces to extrude the upper dentition, thereby rotate the mandible in a clockwise direction for improved facial esthetics and mandibular prognathism.[9]
This case report presents the correction of a skeletal class III malocclusion by rotating the Maxillo-Mandibular complex(MMc) in a clockwise direction to achieve clinically acceptable treatment outcome and favourable facial esthetics in an adult patient.
Case Report
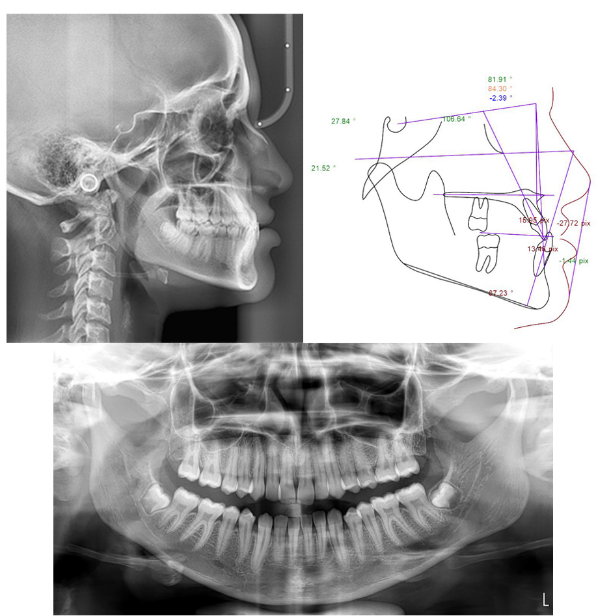
A female patient of 18 years old reported with the chief complaint of dissatisfied smile and facial appearance. Facial examination revealed that she was having horizontal growth pattern, concave profile, anterior divergent face, prominent chin and laterocclusion of mandible towards left side with Centric Relation (CR)-Centric Occlusion(CO) discrepancy. The maxilla was retrognathic with relative mandibular prognathism and the incisor display and smile line was compromised due to vertical maxillary deficiency. Intraoral examination revealed that she had anterior crossbite, Angles Class III malocclusion with dental compensations and mandibular dental midline shifted towards left side by 3mm ([Figure 1]). Pre-treatment cephalometric analyses are given in [Table 1] and ([Figure 2]).
Problem list
Skeletal problem
Skeletal Class III Base
Sagittal and Vertical Maxillary deficiency
Relative mandibular prognathism
Hypodivergent face
Dental problem
Class III molar relationship
Mild crowding of maxillary anteriors
Anterior crossbite
Lingually placed mandibular right lateral incisor
Laterocclusion and Midline shift
Soft tissue problems
Concave profile
Obtuse nasolabial angle
Positive lip step
Chin prominence
Compromised incisor display and smile arc
Treatment objectives
Alignment and levelling of upper and lower arches
Correction of anterior crossbite
To achieve Class I molar relationship
Correction of dental midline shift
Improvement of maxillary incisor visibility
Improvement of smile arc
Treatment alternatives
The success of orthodontic treatment is not just to achieve the treatment goals, but also to fullfill patient’s expectations with maximum benefit and minimum cost and risk10. As the patient had a moderate skeletal Class III problem with horizontal growth pattern, maxillary sagittal and vertical deficiency, an orthodontic camouflage was chosen as the treatment plan. Total arch distalization of the mandibular dentition with mini implants was an alternative, but considering the risk of excessive retraction of lower anteriors and possible increase of chin prominence, that plan was discarded. Fixed appliance therapy with Class III intermaxillary elastics could also have been a choice to increase the vertical dimension, but this procedure would rotate the occlusal plane in counterclockwise direction and thereby further procline the upper anteriors and compromise smile arc. The strategy of the mechanics in the present case was to extrude of the maxillary dentition resulting in clockwise rotation of the mandible and reduction of chin prominence as advocated by Eric Liou.[9]
Mechanotherapy
The case was started with Pre adjusted Edgewise Appliance, 0.022” x 0.028” MBT prescription and the strap up included second molars in both arches. After initial alignment levelling of the arches, a TPA was incorporated in the maxillary arch to hold the molar segments and 0.018 round stainless steel wires were placed which was segmented mesial to first molars. A continuous 0.019x0.025 rectangular stainless steel wire was placed in the mandibular arch for increased stability. Bite raisers were placed using light cure composite (Blue bite)on the occlusal surface of maxillary first molars so that 2 to 3mm bite was opened on the incisor region. Intermaxillary vertical elastics with force range of 200-250 gms were advised to wear from maxillary anterior segment to mandibular arch to facilitate extrusion of maxillary dentition mesial to first molars([Figure 3]).
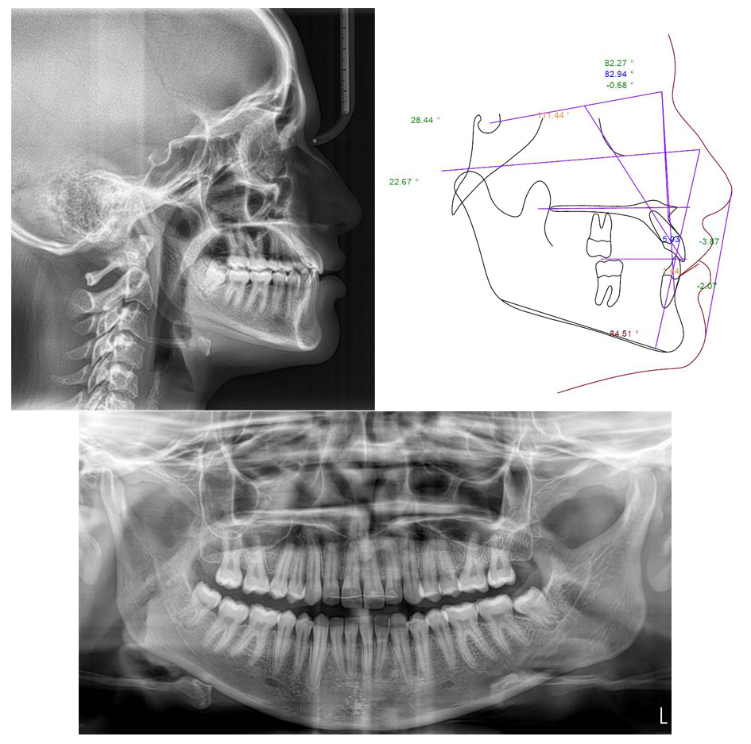
Once the upper anterior segment has occluded with the lower arch, bite raisers and TPA were then removed and a continuous 0.018 round Niti arch wire placed in the maxillary arch. Intermaxillary vertical elastics were advised to continue for the extrusion of maxillary posterior segment([Figure 4]). Once the maxillary posterior teeth were occluded with mandibular arch, a continous rectangular 0.019x0.025 Niti followed by Stainless steel wire was placed in the upper arch for expression of tip and torque. The occlusion was settled with settling elastics and the case was finished with satisfactory post treatment facial and occlusal outcome([Figure 5]). The post treatment cephalometric analysis are showed in Table.I and ([Figure 6])
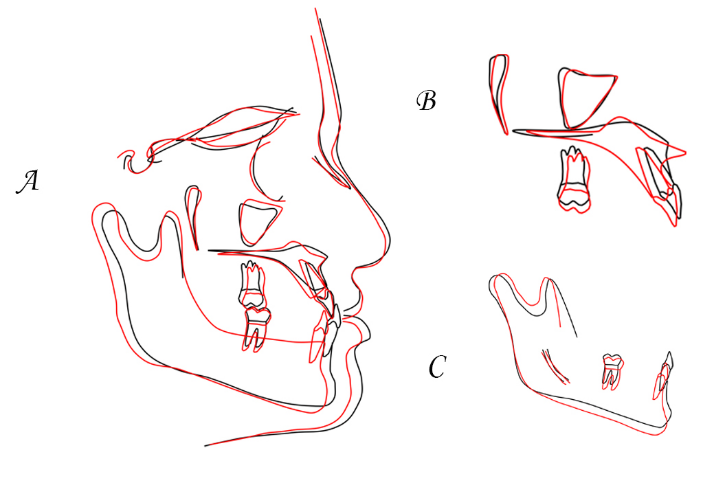
The pre-treatment and post-treatment cephalograms were superimposed to assess the changes as per the American Board of Orthodontics(ABO) cephalometric superimposition criteria on the anterior cranial base, maxilla and mandible. The cranial base superimposition was done based on the plane constructed by anterior wall of sella tursica and cribriform plate(SNL) to assess the overall treatment changes of maxilla, mandible, maxillary dentition and mandibular dentition. Maxillary superimposition was assessed by taking the anterior contour of zygomatic process as the stable structure and mandibular superimposition was done by taking the mandibular canal as the stable landmark([Figure 7]). The super impositions were assessed for the sagittal and vertical changes of maxillo-mandibular complex by evaluating skeletal, dental and soft tissue parameters like Point A, Point B, Pogonion, Menton, SN - Occlusal plane, SN – Mandibular plane, maxillary incisor, maxillary molar, mandibular incisor, mandibular molar, upper lip to E-line, lower lip to E-line, soft tissue pogonion and menton ([Table 2]).
Results
The findings of the post treatment records revealed that favourable changes occurred for the correction of Class III malocclusion. The maxillary dentition was moved down and anteriorly along with rotation of mandible in a clockwise direction(28.7degrees) which is evident on the increase of mandibular plane(22.7 degrees). The maxilla moved anteriorly(SNA-82.3 degree), mandible moved posteriorly(SNB-82.9 degree) and the maxillo-mandibular relation in sagittal plane was improved(ANB value 1.7 mm) suggesting the achievement of Class I molar relationship and a positive overjet. This change was mainly occurred due to backward movement of Point. B(1.4 degree) and forward movement of Point A(0.4mm).
The cephalometric superimposition revealed forward and downward movement of maxilla, maxillary dentition, backward and downward movement of mandible and mandibular dentition which resulted in reduction of chin prominence and favourable profile changes([Table 2]). Although there was not much changes observed in the skeletal parameters of maxilla (Pt. A moved only 1 mm downwards), there was definite changes in mandible(Pt.B, Pog and Me moved back by 4mm each and downward by 2,5 and 4mm respectively). The SN-Occl plane and SN-Mand plane also increased by 2 degrees which is the result of clockwise rotation. The dentition also showed favourable changes which is evident in movement of upper incisors and molars moved downwards by 2 mm each and lower incisors and molars backwards and downwards by 5mm, 3mm and 2 mm respectively. Upper lip moved forward and downward by 2mm each and lower lip moved back by 3mm and down by 2mm which is a favourable result. Favourable soft tissue changes were noticed with Pogonion and menton also by backward movement of 4mm each and downward movement by 3mm each.




|
Parameters |
Normal |
Pre-Treatment |
Post-Treatment |
Difference |
|
Skeletal |
||||
|
SNA(degree) |
82 |
81.9 |
82.3 |
0.4 |
|
SNB (degree) |
80 |
84.3 |
82.9 |
-1.4 |
|
ANB (degree) |
2 |
-2.4 |
-0.7 |
-1.7 |
|
SN-MP (degree) |
32 |
27.8 |
28.7 |
0.9 |
|
FMA (degree) |
25 |
21.5 |
22.7 |
1.2 |
|
Dental |
||||
|
Upper 1 to NA(mm) |
4 |
16 |
5 |
11 |
|
Upper 1 to SN (degree) |
103 |
106.6 |
111.4 |
4.8 |
|
Lower 1 to NB (mm) |
4 |
13.5 |
1.4 |
12.1 |
|
Lower 1 to MP (degree) |
95 |
87.2 |
84.5 |
2.7 |
|
Overjet (mm) |
3.5 |
-7.4 |
2.9 |
10.3 |
|
Overbite (mm) |
2 |
17 |
2 |
15 |
|
Soft Tissue |
||||
|
Upper Lip to E Line (mm) |
-4 |
-27.7 |
-3.9 |
-23.8 |
|
Lower Lip to E-Line (mm) |
-2 |
-1.4 |
-2.1 |
-0.7 |
|
|
Variables |
Sagittal (mm) |
Vertical (mm) |
|
Skeletal |
Pt A |
-1 |
+1 |
|
Pt B |
-4 |
+2 |
|
|
Pog |
-4 |
+5 |
|
|
Me |
-4 |
+4 |
|
|
SN-OP (Degree) |
|
+2 |
|
|
SN-MP(Degree) |
|
+2 |
|
|
Dental |
U-1 |
-1 |
+2 |
|
L-1 |
-5 |
+3 |
|
|
U-6 |
+2 |
+2 |
|
|
L-6 |
0 |
+1 |
|
|
Soft tissue |
UL-E Line |
+2 |
+2 |
|
LL-E Line |
-3 |
+2 |
|
|
Pog |
-4 |
+3 |
|
|
Me |
-4 |
+3 |
Discussion
Occlusal plane regulation by differential tooth movement produced by extra oral appliances, intra oral fixed appliances with springs and intermaxillary elastics has been documented in the literature.[10], [11] Orthodontic camouflage by clockwise rotation of the maxillo-mandibular complex represents a new treatment modality in borderline skeletal Class III malocclusions.[7], [8] This case report represents the correction achieved by clockwise rotation of maxillo-mandibular complex with fixed appliance in a Class III non-growing patient. The decision of whether to perform surgical or non-surgical treatment in borderline skeletal Class III cases depends on the case selection. The severity of skeletal discrepancy, degree of incisor compensations, facial growth pattern, periodontal status, anterior facial proportions and esthetic appearance are important factors to be considered.[12], [13]
Many investigators documented the discriminative factors in determining whether the Class III malocclusion should be treated by surgery or orthodontic camouflage.[14], [15] Surgery is almost always indicated when the ANB angle less than -4 degree, IMPA is below 83 degrees and a higher negative Wits appraisal. In our patient, ANB angle was -2.4 degree, IMPA was 87.2 degree and -3 mm of Wits appraisal which showed that the case was ideally suitable for an orthodontic camouflage.
The treatment option in our patient was chosen due to clinical criterias like borderline skeletal Class III with maxillary deficiency, decreased smile display with vertical anterior maxillary deficiency, hypo divergent facial growth pattern and functional shift of mandible which was evident on CO-CR discrepancy. Increase of vertical dimension by Class III intermaxillary elastics with fixed appliance was another option, but retraction of lower incisors would have further increased the chin prominence resulting in an unesthetic outcome. Not only that class III elastics retrocline lower incisors and procline upper incisors, this mechanics will extrude the maxillary molars down and mandibular incisors up causing the occlusal plane to rotate in a counterclockwise manner which would further compromise the smile arc in this case.[16] Orthodontic camouflage in many Class III cases addresses the sagittal problems, but seldom on the improvement of vertical deficiency.[15], [17], [18] The extrusion of maxillary arch obtained in our case developed the alveolar vertical bone height and subsequently improved the incisor visibility and smile arc as reported previously.[19] The clockwise rotation achieved with the mandible was due to extrusion of maxillary and mandibular dentition which was advantageous in increasing the growth pattern, reduction in chin prominence and improving smile arc as proposed by Eric Liou et al.[9] Extrusion of maxillary dentition in the anterior segment initially was another advantage in this case as it improved the smile features and bite raisers in the maxillary molar region prevented the extrusion and thereby tipping the occlusal plane in a clockwise manner.
Conclusion
Orthodontic clockwise rotation of Maxillo-Mandibular complex (MMc) is an effective and satisfactory strategy to treat mild to moderate skeletal Class III malocclusions in young and non-growing patients. This modality of treatment is indicated in patients with short face, vertical maxillary deficiency, low mandibular plane and minimum dental compensations. The extrusion of maxillary and mandibular dentition resulted in improved facial balance, acceptable profile and smile esthetics with stable occlusion.
Source of Funding
None.
Conflict of Interest
None.
References
- A Venugopal, P Manzano, N Vaid. TAD driven Class III camouflage: Eight point protocol to optimize efficiency, aesthetics and stability. Sem Orthod 2022. [Google Scholar]
- MA Bittencourt. Early treatment of patient with Class III skeletal and dental patterns. Dental Press J Orthod 2015. [Google Scholar]
- JD Kama, T Ozer, S Baran. Orthodontic and orthopaedic changes associated with treatment in subjects with Class III malocclusions. Eur J Orthod 2006. [Google Scholar]
- JH Park, M Emamy, SH Lee. Adult skeletal class III correction with camouflage orthodontic treatment. Am J Orthod Dentofac Orthop 2019. [Google Scholar]
- BA Troy, S Shanker, HW Fields, K Vig, W Johnston. Comparison of incisor inclination in patients with Class III malocclusion treated with orthognathic surgery or orthodontic camouflage. Am J Orthod Dentofac Orthop 2009. [Google Scholar]
- HS Baik. Limitations in orthopaedic and camouflage treatment for Class III malocclusion;. Sem Orthod 2007. [Google Scholar]
- RSJP Reyneke, R Bryant, PJ Suuronen. Post operative skeletal stability following clockwise and counterclockwise rotation complex compared with conventional orthognathic treatment. Br J Oral Maxfac Surg 2007. [Google Scholar]
- IM Tsai, CH Lin, YC Wang. Correction of skeletal class III malocclusion with clockwise rotation of the maxillomandibular complex. Am J Orthod Dentofac Orthop 2012. [Google Scholar]
- JW Eric, Yu-Chi Liou. Orthodontic clockwise rotation of maxillomandibular complex for improving facial profile in late teenagers with Class III malocclusion: A preliminary report. APOS Trends Orthod 2018. [Google Scholar]
- FW Worms, RJ Isaacson, RM Spiedel. A concept and classification of rotation and external force systems. Angle Orthod 1973. [Google Scholar]
- U Teuscher. An appraisal of growth and reaction to extra oral anchorage. Am J Orthod 1986. [Google Scholar]
- HS Baik, HK Han, DJ Kim, WR Proffit. Cephalometric characteristics of Korean Class III surgical patients and their relationship to plans for surgical treatment. Int Adult Orthod Orthognath Surg 2000. [Google Scholar]
- HS Baik. . Limitations of Orthopedic Treatment and Combined Surgery in Skeletal Class III Malocclusion. Orthodontics in the 21st Century 2002. [Google Scholar]
- WJS Kerr. Class III malocclusions: Surgery or Orthodontics. Br J Orthod 1992. [Google Scholar]
- AS Eisenhauer, CJ Lux, G Schuster. Treatment decision in adult patients with Class III malocclusion: orthodontic therapy or orthognathic surgery?. Am J Orthod Dentofac Orthop 2002. [Google Scholar]
- KR Chung, SH Kim, YA Kook. C-orthodontic microimplant for distalization of mandibular dentition in Class III correction. Angle Orthod 2005. [Google Scholar]
- NR Burns, DR Musich, C Martin, T Razmus, E Gunel, P Ngan. Class III camouflage treatment: What are the limits?. Am J Orthod Dentofac 2010. [Google Scholar]
- PD Tekale, KK Vakil, SM Parhad. Orthodontic camouflage in skeletal class III malocclusion: A contemporary review. J Orofac Res 2014. [Google Scholar]
- EY Kwon, JY Lee, J Choi. Effect of slow forced eruption on the vertical levels of the interproximal bone and papilla and the width of the alveolar ridge. Korean J Orthod 2016. [Google Scholar]