- Visibility 31 Views
- Downloads 14 Downloads
- DOI 10.18231/j.jco.2024.010
-
CrossMark

Evaluation of orthodontic treatment need in school children of shimla using index of orthodontic treatment need
- Author Details:
-
 Sonia Chauhan *
Sonia Chauhan *
-
K. S. Negi
-
Nishant Negi
Introduction
Maintenance of good health is of prime importance to any individual. Oral health is one of the important component of a healthy life. For orthodontic treatment to become an integral part of oral health care programs, basic information on treatment needs is required.
Developing countries like India has also shown an increase in demand for orthodontic treatment as people are becoming more aware about oral health conditions and subsequent care available. Logical planning of orthodontic treatment on population basis is important. Patient with treatment need should be addressed first and while those with little need can be protected from unnecessary intervention.
The Occlusal Index[1] the Treatment Priority Index[2] assess malocclusion but do not take the soft tissue profiles or facial asymmetries into account. The Swedish Dental Society and the Swedish Medical Board. [3] developed an index which classified malocclusion into grades but these grades were not well-defined and the cut-off points were somewhat vauge.[4] Brook and Shaw in 1989[5] introduced the Index of Orthodontic Treatment Need which categorises malocclusion into distinct categories of treatment need and also includes a measure of function.[6]
The IOTN incorporates both a dental health component and an aesthetic component. The DHC represents biological or anatomical aspects of IOTN that records need for treatment on dental health and functional grounds. The AC measures aesthetic impairment and justifies treatment on social-psychological grounds.
Objectives
The objective of this survey was to gauge the orthodontic treatment need in school children of Shimla, Himachali Pradesh, India aged 12- 16 years using Index of Orthodontic Treatment Need, determine the orthodontic treatment need in males and females, to judge the subjects knowledge and demand for orthodontic treatment, compare orthodontist’s perception of treatment need with that of subjects and to find correlation between DHC and AC of Index of Orthodontic Treatment Need.
Materials and Methods
This study will be carried out in Shimla, Himachal Pradesh. Adequate number of 12-16 years old school children will be examined and analysed using Index of Orthodontic Treatment Need.
Inclusion criteria
Children aged between 12 to 16 years.
Children studying in school of Shimla, Himachal Pradesh.
Exclusion criteria
Children who were undergoing or had undergone orthodontic treatment.
Children with any congenital anomalies.
Data collection
An intraoral examination of the participating students was conducted in the selected school compound after following the infection control procedures. Frontal intra-oral photographs in centric occlusion were taken after applying cheek retractors with high resolution digital camera. The subjects were evaluated using the Dental Health Component ([Table 1]).
|
Grade 1: No treatment |
|
|
|
Extremely minor malocclusion with contact point displacement of less than 1 mm |
|
Grade 2: Minor anomaly, no treatment need |
|
|
2a |
Overjet > 3.5 mm and ≤ 6 mm (with competent lip closing). |
|
2b |
Reverse overjet between 0 and ≤ 1mm. |
|
2c |
Anterior or posterior crossbite with 1 mm disrepency between Retruded Contact Position and intercuspal position. |
|
2d |
Contact point displacement > 1 mm and ≤ 2 mm. |
|
2e |
Anterior or posterior open bite > 1 mm and ≤ 2 mm. |
|
2f |
Increased overbite of ≥ 3.5 mm (without gingival contact). |
|
2g |
Class II or Class III occlusal without other anomalies (up to half a premolar width). |
|
Grade 3: Borderline treatment need |
|
|
3a |
Overjet > 3.5 mm and < 6 mm (incompetent lip closing). |
|
3b |
Reverse overjet between 1 and ≤ 3.5 mm. |
|
3c |
Anterior or posterior crossbite with > 1 mm and ≤ 2 mm discrepancy between RCP and ICP. |
|
3d |
Contact point displacements > 2 mm and ≤ 4 mm. |
|
3e |
Lateral or anterior open bite > 2 mm and ≤ 4 mm. |
|
3f |
Deep overbite with gingival contact or contact with palatal mucosa (but without trauma). |
|
Grade 4: Treatment need |
|
|
4h |
Less severe hypodontia. |
|
4a |
Overjet > 6 mm and ≤ 9 mm. |
|
4b |
Reverse overjet > 3.5 mm (without masticatory or speech problems). |
|
4m |
Reverse overjet > 1 mm and ≤ 3.5 mm (without masticatory or speech problems). |
|
4c |
Anterior or posterior crossbite with > 2 mm discrepancy between RCP and ICP. |
|
4l |
Posterior lingual crossbite with no functional occlusal contact in one or both buccal segments. |
|
4d |
Major contact point displacement > 4 mm. |
|
4e |
Extreme lateral or anterior open bite > 4 mm. |
|
4f |
Increased and complete overbite with gingival or palatal trauma. |
|
4t |
Partially erupted teeth, tipped and impacted against adjacent teeth. |
|
4x |
Existence of supernumerary teeth. |
|
Grade 5: Treatment need |
|
|
5i |
Impeded tooth eruption (3rd molars) attributable to crowding, displacements, supernumerary teeth, retained deciduous teeth. |
|
5h |
Extensive hypodontia (more than 1 congenitally missing tooth). |
|
5a |
Increased overjet > 9 mm. |
|
5m |
Reverse overjet > 3 mm with masticatory problems and speech disorders. |
|
5p |
Cleft lip and palate and other craniofacial anomalies. |
|
5s |
Retained deciduous teeth. |
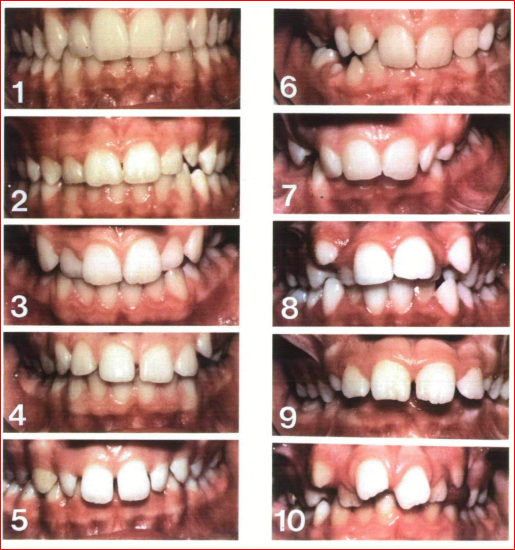
To record the Aesthetic component, the SCAN index (Standardized Continuum of Aesthetic Need) was used (Evans and Shaw, 1987)[7] ([Figure 1]). The subjects will be made to observe their own teeth in the mirror without cheek retractors and compare them with one of the 10 coloured photographs. Grade 1 was assigned to aesthetically optimal dentition while grade 10 was assigned to the worst imaginable dentition. All subject’s intraoral photographs were also evaluated by an orthodontist using the same grades.
The subjects were allocated to different treatment categories for Dental Health Component ([Table 2]) and Aesthetic Component ([Table 3]).
|
Grade 1-2 |
No treatment need |
|
Grade 3 |
Borderline treatment need |
|
Grade 4-5 |
Treatment Need |
|
Grade 1-4 |
No treatment need |
|
Grade 5-7 |
Borderline |
|
Grade 8-10 |
Treatment need |
Statistical analysis
Data analysis was performed using Statistical Package for Social Science Version 20. The results for orthodontic treatment need were expressed in percentages. χ² test of independence was applied to compare the difference in orthodontic treatment need for males and female and for comparing the orthodontist and subjects perception of orthodontic treatment need. Pearson’s correlation was applied to assess the correlation between the Dental Health Component and Aesthetic Component of IOTN and the knowledge and demand of orthodontic treatment need was calculated using 5 point Likert scale statistical significance set at P < 0.05.
Results
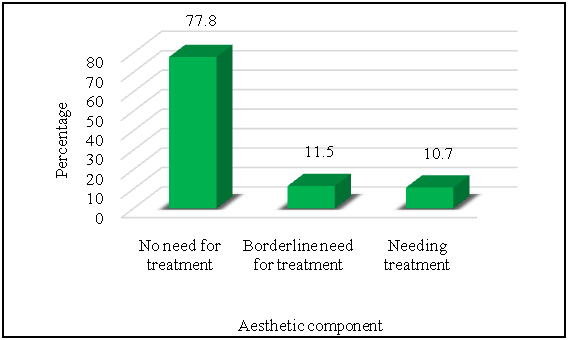
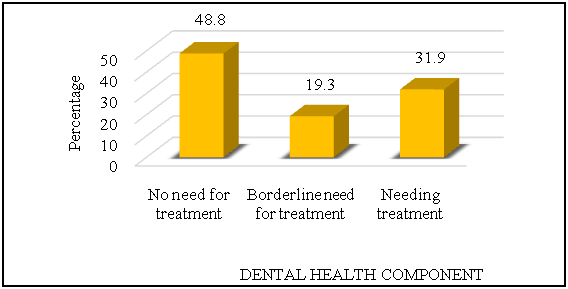
273 males and 303 females were surveyed. Assessment based on Aesthetic component ([Figure 2]) showed that 77.8% (448) of the subjects had no need for orthodontic treatment. 11.5% (66) had borderline need and 10.7% (62) had definite need for orthodontic treatment. Similarly, on assessing the Dental Health Component ([Figure 3]) for the same number of children 48.8% (281) had no need for orthodontic treatment, 19.3% (111) had borderline need while 31.9% (184) had definite need for orthodontic treatment.
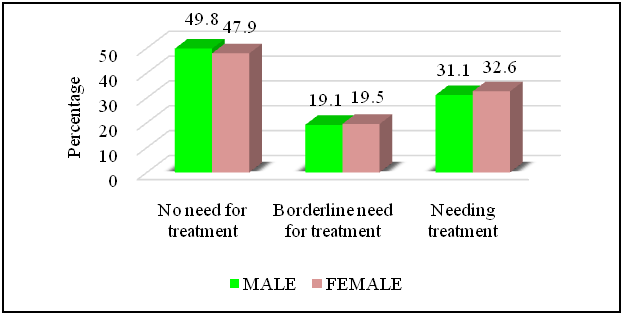
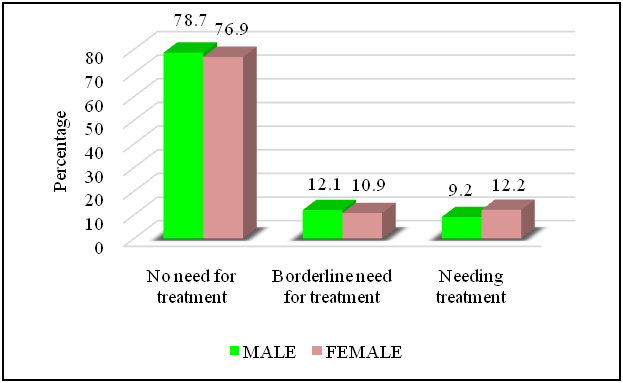
The difference in the grades of Aesthetic component and Dental health component between male and female was not statistically significant. ([Figure 4], [Figure 5])
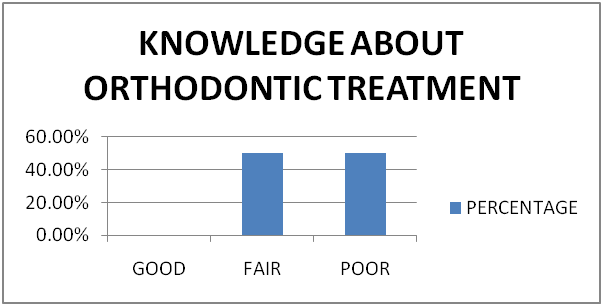
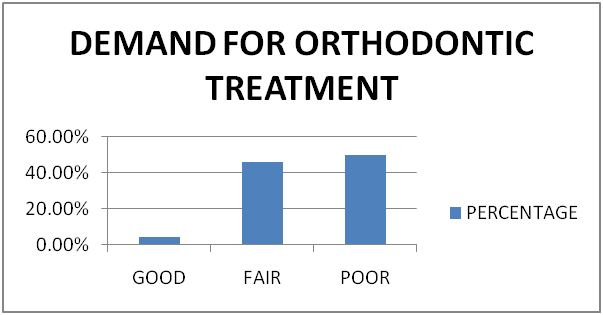
Based on a questionnaire the knowledge of the subject about orthodontic treatment was assessed and only 0.5% (3) subjects had good knowledge while 49.7% (286) subjects had fair knowledge. 49.8% (287) of the subjects had poor knowledge about orthodontic treatment ([Figure 6]). 4.4% (25) subjects had good demand while 45.8%(264) subjects had fair demand and 49.8% (287) of the subjects had poor knowledge about orthodontic treatment ([Figure 7]).
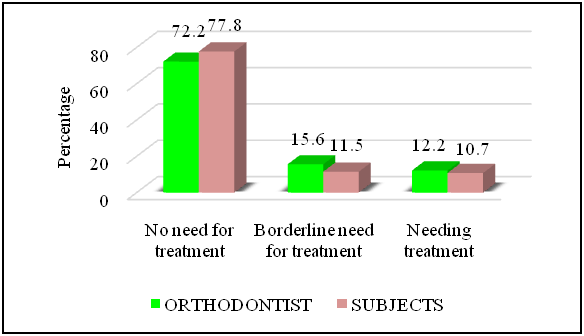
10.7% (62) of the subjects sensed need for orthodontic treatment. For the same category examiner perceived a treatment need of 12.2% (70) for the subjects ([Figure 8]). The value of χ² = 445.17 indicated the degree of difference between each category values and a p value of 0.000 indicated that this difference is statistically significant.
The value of Pearson correlation r=0.636 indicates a strong and positive correlation between DHC and AC of IOTN which is statistically significant.
Discussion
Different countries have adopted varying methods of funding orthodontic care for children. In countries that embrace the principle of publicly funded orthodontic care for all children with high objective need, reliable population data are required to evaluate the effectiveness of the orthodontic services.
The present study was conducted on 576 school children in the age group of 12-16 years in Shimla, Himachal Pradesh, India. The subjects aged 12-16 years were chosen because they have all or almost all their anterior teeth erupted and this age group represents the period of eruption of permanent teeth when most potential orthodontic problems become evident. Adolescent above 12 years of age were capable of abstract thinking, reasoning about timings of past events and correlating them with good and bad experiences.
Children belonging to this age group had higher expectations of self-image enhancement after orthodontic treatment and this might have influenced their esthetics self-perception. Some patients were concerned about minor malocclusions and demanded orthodontic intervention whereas others accepted a major deviation from the norm quiet happily because it did not had a negative impact on daily living.
The definite need for orthodontic treatment assessed by Dental Health Component of IOTN for the present study was 31.9% which was close to the findings of Brook and Shaw[7] (32.7%) and other studies.[8], [9], [10], [11]
According to the present study conducted on school children 77.8% had no/little need for treatment, 11.5% had borderline need and 10.7% had the definite need for orthodontic treatment as assessed by the Aesthetic Component. Similar findings were reported in other studies.[12], [13], [14]
The reason for this difference could probably be that Aesthetic component was obtained from aesthetic impact perceived by the children themselves rather than by the orthodontist. The aesthetic component of IOTN, like the DHC, was quick and easy for the examiner to use. In contrast the children, in some cases, found the concept behind the Aesthetic component difficult to grasp. Children constantly attempted to match their dentition to the photographs, looking for specific morphological traits. This was especially true for children with fractured incisors, bilaterally congenitally absent or peg-shaped lateral incisors, open bite, reverse overjet and Class III malocclusion, all of whom found difficulty in the selection of a photograph which best represented their degree of dental attractiveness.
The difference in the grades of dental health component and aesthetic component between male and female was statistically insignificant (p=0.890). These findings are similar to others.[15], [16], [17]
The main factors for not undergoing orthodontic treatment by patients are lack of awareness, the inadequacy of sources, literacy rate and socio-economic status. According to the present study 50.2% of the subjects had good knowledge about the orthodontic treatment while 49.8% had poor knowledge. They had seen someone with braces or had heard about correction of crooked teeth with braces. This was more than as reported in others studies.[17], [18], [19]
The demand for orthodontic treatment is complex, subjective and varies greatly between individuals. Gender, socioeconomic background and age affects demand for orthodontic treatment. The demand for orthodontic treatment among school children was 50.2% (289) which was similar to the earlier studies. [20], [21], [22]
10.8% (62) of the subjects perceived need for orthodontic treatment. For the same category examiner perceived a treatment need of 12.2% (70) for the subjects. The difference between examiner and subjects was statistically significant (p=0.000). This indicated that children were less critical in their aesthetic evaluation than professionals. Similar finding had been reported in earlier studies.[7], [9], [23], [24]
Self-image of the subjects on seeing the photos of malocclusion revealed that a majority of subjects 77.8% (448) perceived themselves to be in AC grade 1–2 indicating no treatment need. The subjects were intuitively assigning themselves on the appealing side. However, this was opposite to the answers in the questionnaires responded by the subjects.
The imbalance of treatment need using AC and expressed demand could be due to the fact that AC photos were two-dimensional in nature and sagittal or vertical discrepancies could not be appreciated by the children in the photos. Examiner also placed a majority of subjects (77.2%) in grade 1–2 indicating no treatment need.
A positive correlation (r=0.636) was observed between Dental Health Component and Aesthetic Component of IOTN which was statistically significant(p=0.000). These findings were in accordance with other studies.[15], [17], [25], [26]
A lack of agreement between treatment needs according to AC and DHC of the IOTN may be because of the fact that malocclusion traits such as missing teeth, contact point displacement and cross-bites of posterior teeth do not always have an impact on attractiveness of dentition.[11] There is a tendency to score higher for dental attractiveness and less for orthodontic treatment when seeing photographs.[27]
The inconsistency between AC and DHC of IOTN could be clarified on the basis that dental features such as irregularly placed teeth in the lower arch, increased overjet, missing posterior teeth and impacted canines could not be figured on the anterior aspect of photos of AC which placed them in “no treatment need” category.
The findings of the present study led to the conclusion that specific treatment need is widespread when determined according to morphologic criteria in contrast to when only esthetic criteria are considered. Similar results have been reported by earlier studies.[5], [21], [23], [28]
Conclusion
31.9% (184) and 10.8% (62) of the schoolchildren had definite need for orthodontic treatment according to the Dental health component and aesthetic component of index of orthodontic treatment need respectively. 49.7% (286) of the subjects had knowledge about orthodontic treatment. 45.8% (264) of the subjects expressed desire to undergo orthodontic treatment. Orthodontist was more critical in aesthetic evaluation as compared to the school children.
Source of Funding
None.
Conflict of Interest
None.
References
- CJ Summers. The occlusal index: a system for identifying and scoring occlusal disorders. Am J Orthod 1917. [Google Scholar]
- . Orthodontic treatment Priority Index. National Center for Health Statistics. Public Health Service Publication No. 1000-Series 2 no.25. 1967. [Google Scholar]
- S Linder-Aronson. Orthodontics in the Swedish Public Dental Health Service. Trans Eur Orthod Soc 1974. [Google Scholar]
- WC Shaw, S Richmond, KD O’brien, P Brook, CD Stephens. Quality control in orthodontics: indices of treatment need and treatment standards. Br Dent J 1991. [Google Scholar]
- PH Brook, WC Shaw. The development of an index of orthodontic treatment priority. Eur J Orthod 1989. [Google Scholar]
- S Cooper, N A Mandall, D Dibiase, WC Shaw. The reliability of the Index of Orthodontic Treatment Need Over time. J Orthod 2000. [Google Scholar]
- MR Evans, WC Shaw. Preliminary evaluation of an illustrated scale for rating dental attractiveness. Eur J Orthod 1987. [Google Scholar]
- S Richmond, M Andrews. Orthodontic treatment standards in Norway. Eur J Orthod 1993. [Google Scholar]
- A Holmes. The Subjective Need and Demand for Orthodontic Treatment. Br J Orthod 1992. [Google Scholar]
- IB Buchanan, A Downing, DR Stirrups. A Comparison of the Index of Orthodontic Treatment Need Applied Clinically and to Diagnostic Records. Br J Orthod 1994. [Google Scholar]
- DJ Burden, A Holmes. The need for orthodontic treatment in the child population of the United Kingdom. Eur J Orthod 1994. [Google Scholar]
- S Sultana, Z Hossain. Prevalence and factors related to malocclusion, normative and perceived orthodontic treatment need among children and adolescents in Bangladesh. Dental Press J Orthod 2019. [Google Scholar]
- NA Mandall, JF McCord, AS Blinkhorn, HV Worthington, KD O'Brien. Perceived aesthetic impact of malocclusion and oral self-perceptions in 14-15-year-old Asian and Caucasian children in greater Manchester. Eur J Orthod 2000. [Google Scholar]
- P Kumar, SM Londhe, A Kotwal, R Mitra. Prevalence of malocclusion and orthodontic treatment need in schoolchildren - An epidemiological study. Med J Armed Forces India 2013. [Google Scholar]
- N Ucuncu, E Ertugay. The use of the Index of Orthodontic Treatment need (IOTN) in a school population and referred population. J Orthod 2001. [Google Scholar]
- M Souames, F Bassigny, N Zenati, PJ Riordan, ML Boy-Lefevre. Orthodontic treatment need in French schoolchildren: an epidemiological study using the Index of Orthodontic Treatment Need. Eur J Orthod 2006. [Google Scholar]
- PI Ngom, F Diagne, F Dieye, K Diop-Ba, F Thiam. Orthodontic treatment need and demand in Senegalese school children aged 12-13 years. An appraisal using IOTN and ICON. Angle Orthod 2007. [Google Scholar]
- K Chaitra, N Reddy, S Reddy, Vanishree. Orthodontic treatment: need and demand in north Karnataka school children. J Clin Diagn Res 2014. [Google Scholar]
- M Pandey, J Singh, Mangal, P Yadav. Evaluation of awareness regarding orthodontic procedures among a group of preadolescents in a cross-sectional study. J Int Soc Prev Community Dent 2014. [Google Scholar]
- WC Shaw. Factors influencing the desire for orthodontic treatment. Eur J Orthd 1981. [Google Scholar]
- ESJA Alhaija, KS Al-Nimri, SN Al-Khateeb. Orthodontic treatment need and demand in 12-14-year-old north Jordanian school children. Eur J Orthod 2004. [Google Scholar]
- N Singh, D Bagga, R Sharma, R Singh. Evaluation of reliability of index of orthodontic treatment need for assessment of orthodontic treatment need. Int J Orthod Rehabil 2017. [Google Scholar]
- K Birkeland, OE Bøe, P Wisth. Orthodontic concern among 11-year-old children and their parents compared with orthodontic treatment need assessed by Index of Orthodontic Treatment Need. Am J Orthod Dentofacial Orthop 1996. [Google Scholar]
- ESJA Alhaija, KS Al-Nimri, SN Al-Khateeb. Self-perception of malocclusion among north Jordanian school children. Eur J Orthod 2005. [Google Scholar]
- AA Dogan, E Sari, E Uskun, AMS Sağlam. Comparison of orthodontic treatment need by professionals and parents with different socio-demographic characteristics. Eur J Orthod 2010. [Google Scholar]
- CGA Nobile, M Pavia, L Fortunato, IF Angelillo. Prevalence and factors related to malocclusion and orthodontic treatment need in children and adolescents in Italy. Eur J Public Health 2007. [Google Scholar]
- JM Sherlock, MT Cobourne, F Mcdonald. Assessment of orthodontic treatment need: a comparison of study models and facial photographs. Community Dent Oral Epidemiol 2008. [Google Scholar]
- E Josefsson, K Bjerklin, R Lindsten. Malocclusion frequency in Swedish and immigrant adolescents--influence of origin on orthodontic treatment need. Eur J Orthod 2007. [Google Scholar]