- Visibility 89 Views
- Downloads 12 Downloads
- DOI 10.18231/j.jco.2024.013
-
CrossMark

Correction of class II malocclusion with modified pendulum appliance – A case report
- Author Details:
-
 Abrar Younus A *
Abrar Younus A *
-
Nausheer Ahmed
-
Nishat Sidiqha
-
Chethana Prabhakar
-
Uroosa Aymen
Introduction
Molar distalization has become a highly prevalent procedure to correct class two malocclusions as a result of the recent paradigm change toward the non-extraction approach. Non-extraction treatment has also grown increasingly popular in the correction of Class II malocclusions. One of the most popular non-extraction methods for treating Class II malocclusion is the distalization of maxillary molars.
The focus has been on creating therapy methods and equipment that treat malocclusions without requiring patient participation throughout the last few decades. Intra-arch devices for molar distalization have been developed as a primary method to non-compliance appliances.[1] Several Appliances, such as the Pendulum appliance and repelling magnets [2], [3] Wilson Bimetric Distalizing Arch (BDA),5 Acrylic Cervical Occipital Appliance (ACCO),K-loop, Jasper jumper, and Distal jet have all shown promising clinical outcomes. [4], [5], [6] Premolar extrusion, mesial displacement of the mandibular teeth, and flare of the front teeth are only a few of the negative reciprocal consequences that practically all of the appliances exhibit.[7]
Hilgers created the pendulum devices back in 1992. One of the more popular intraoral conventional distalizing gadgets is this one. [8] The pendulum appliance is indicated in cases of mesially drifted upper first molars due to the early loss of primary molars, unilateral or bilateral distalization of maxillary first molar teeth for Class II molar relationship correction in noncompliant patients, and for regaining space. Treatment of mild to moderate crowding without extraction. The main drawbacks of this device include anchoring loss, anterior tooth proclination, and greater overjet, all of which may lengthen treatment times and round the anchor teeth. [9], [10], [7], [11], [12] To reduce anchoring loss, the pendulum appliance recently underwent a number of changes. This contains a modified pendulum appliance [9], [10], [7], [11], [12], [13] a segmented pendulum appliance for the sequential distalization of the second molar, and a quad pendulum for the simultaneous distalization of the second and first molars.
Scuzzo et al. [9] developed a modified pendulum in 1999 that had the horizontal pendulum loop reversed to permit movement of the maxillary molars' roots and crowns. The loop can be activated by opening it following the distal molar movement. Instead of only tilting or rotating, the activation causes the buccal and/or distal uprighting of the molar roots, which enables actual physical movement of the teeth. This case report describes the non-extraction treatment of class II molar relation by distalization into class I molar relation with a modified pendulum appliance. [9]
Diagnosis and Treatment Plan
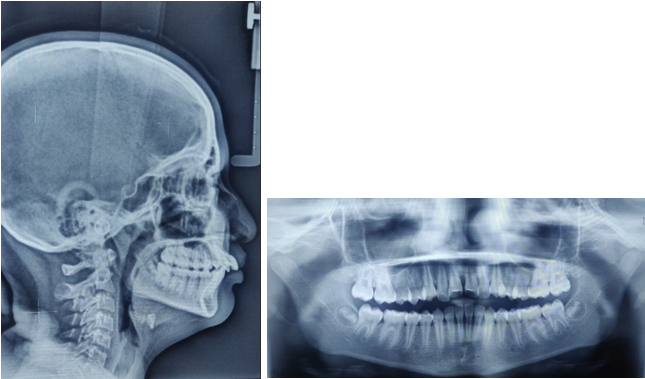
A 12-year-old female patient, presented with the chief complaint of forwardly placed upper teeth and irregular lower front teeth. There was no relevant medical or dental history. On clinical appraisal, no abnormality was detected with the temporomandibular joint. she had a mesoprosopic facial form, slightly convex profile, straight divergence, negative lip step, competent lips, and acute nasolabial angle with no gross facial asymmetry ([Figure 1]).
On examination, she showed an overjet, an overbite, and end-on-molar relation proclined upper incisors on a Skeletal class I base of 5mm and 3mm, respectively. A 2mm crowding and a slight Spee curve could be seen in the lower arch. With the exception of the third molars, all permanent teeth had sprouted. Patient had minor fluorosis and fair periodontal health. [Figure 2]


A panoromic radiograph revealed the absence of the top third molars. ANB on the lateral cephalogram was 3°, and Wits assessment indicates that AO is 1 mm ahead of BO and that the beta angle is 30°, which is indicative of a Class I skeletal connection. A 26° SN-MP angle points to a pattern of horizontal expansion. The patient had naturally inclined lower incisors with L1-MP 97° and proclined maxillary incisors with U1-SN 119°. In [Figure 3]. The maxillary first molar's distal surface and Ricketts' PTV line were separated by 19 mm.
Treatment Objectives
To achieve soft tissue balance and harmony
To correct end-on-molar and canine relation and establish class I buccal relationship
To reduce incisor proclination.
To correct crowding with upper and lower anteriors
To establish normal overjet and overbite segment relation
Treatment plan
To correct the end-on-molar connection and upper incisor proclination, bilateral distalization of the maxillary molars was planned utilizing a modified Pendulum Appliance. The pre-adjusted edgewise appliance (MBT Prescription, 0.022 slots) was then used in fixed appliance therapy. The maxillary first molar's distal surface was 19 mm away from Ricketts' PTV line. Ricketts asserts that the minimum gap at age 12 should be 15 millimeters (plus 3 millimeters for growth). A horizontal development pattern and the lack of an upper third molar may favor distalization.
Treatment progress
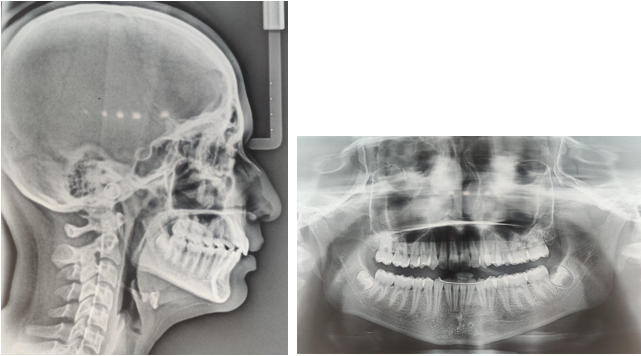
The banded maxillary first molars were fitted with a modified Pendulum appliance with retentive arms on the premolar ([Figure 4]). 90 applied about 220 grams of force to the appliance, turning it on. In order to facilitate the distalization, GIC bite blocks were administered to disocclude the posteriors. The U bend of the pendulum appliance was turned on when the molar began to travel distally, producing physical movement of the teeth. The molars displayed a distal shift of 3.5 mm on the left and 4 mm on the right at the end of four months ([Figure 5]).


Molars were slightly overcorrected to class one relation to counteract any chances of relapse. A mid-treatment orthopantomogram was taken to confirm bodily distalization of the first molar and bone deposition on the mesial aspect of the tooth. After the desired distalization was achieved, the pendulum appliance was removed and the Insta-Nance appliance was delivered on the same day as a means of retention and 0.022×0.028˝ MBT brackets were bonded ([Figure 6]).

The following wire sequence was used to level and align both arches: (a) 0.016 nickel-titanium archwires that are heat-activated (b) 0.018-inch stainless steel archwires; (c) 0.017- to 0.025-inch nickel-titanium archwires. (d) SS archwire, 0.019" x 0.025".
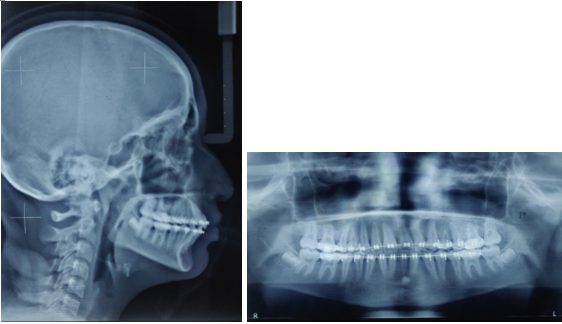
Using an active tie back, the upper anteriors were pulled back. To prevent the proclination of the mandibular and maxillary incisors, the arch wires were tightened distally to the molar. To improve anchoring and correct canine connection, class II elastics were employed on stainless steel wire that was between 0.019 and 0.025 in diameter. Finishing was completed using class two settling elastics on 0.016 nickel titanium archwire. In 18 months, the treatment was finished ([Figure 7]). At the debonding appointment, the patient received a lower fixed retainer and a maxillary Hawley's retainer. The white spot lesion was treated with mouthwash containing fluoride at a low concentration of 0.05%. Every six months, the patient is called back for follow-up, and they are instructed to keep up good oral hygiene.


Cephalometric analysis
|
Skeletal parameters |
Pre-treatment |
Post-treatment |
|
SNA Angle |
82◦ |
80◦ |
|
Point A to Nasion Perpendicular |
2 mm |
1 mm |
|
Condylion to Point A |
74.8 mm |
73.7 mm |
|
SNB Angle |
80◦ |
80◦ |
|
Pogonion to nasion perpendicular |
1 mm |
0 mm |
|
Condylion to Gnathion Perpendicular |
91.3 mm |
95 mm |
|
Wits Appraisal |
3 mm |
0 mm |
|
ANS to Menton |
51.7 mm |
53.9 mm |
|
Frankfort Horizontal Plane to Functional occlusal plane |
12◦ |
13◦ |
|
Frankfort Horizontal Plane to Mandibular plane |
21◦ |
22◦ |
|
Dentoalveolar parameters |
Pre-treatment |
Post-treatment |
|
Overjet |
1.Overjet |
1.Overjet |
|
Overbite |
2.Overbite |
2.Overbite |
|
upper incisor to point A verticle |
3.upper incisor to point A verticle |
3.upper incisor to point A verticle |
|
Lower incisor to mandibular plane |
4.Lower incisor to mandibular plane |
4.Lower incisor to mandibular plane |
|
inter-incisal angle |
98º |
96º |


Discussion
A modified M pendulum appliance was introduced by Scuzzo consisting of the horizontal U loop which is directed mesially rather than distally as in the conventional Hilgers pendulum appliance.[9] It has Two 0.032˝ TMA springs inserted into a 0.036˝ lingual sheath on the maxillary molar bands. The springs are mounted as close to the center and distal edge of the acrylic button as possible to produce a broad, swinging arc (or pendulum) of force. Activation of the pendulum appliance distalises the molars and moves it palatally along an arc with slight distolingual rotation. This has the tendency to produce molar crossbite during diatalization. Activation of the modified U loop not only produces expansion in the molar region, preventing the chances of crossbite but also produces bodily movement of molars.
In this case, the Modified M Pendulum appliance was successfully used for the bilateral distalization of the maxillary first molar into a Class I molar relationship in this case. The presence of a Horizontal growth pattern, missing upper third molars, increased pterygoid vertical to molar distance and the absence of severe crowding all favored the treatment with distalization. The presence of the second molar may influence the distal movement of the first molar, but it remains a matter of debate. Some authors reported that the presence of second molar increases molar tipping, treatment duration, and more anterior anchorage loss. On the contrary, some authors have reported that the presence and the position of the second molar do not affect the amount and the type of maxillary first molar distal movement.[14], [15] Pendulum appliance can produce a molar distalization between 3.14 and 6.1 mm. In our case, 3.5 mm of molar distalization was achieved on the left and 4 mm on the right in the duration of 4 months. Following the distalization phase, an Insta-Nance appliance was placed to stabilize the molar until the retraction of the canine was accomplished. It also facilitated the spontaneous distal drift of the first and second premolars owing to the action of stretched transseptal fibers. Pre and post-treatment superimposition showed there was no significant rotation of the mandibular plane and lower anterior facial height was maintained. Superimposition showed U1 to SN was reduced from 119° to 105° confirming upper incisor retracted. There was no difference in SN-MP suggesting the lower facial height and the mandibular plane remained 26°. L1 to MP was increased from 97° to 99° suggesting lower incisors were slightly proclined during treatment. The distance between pterygoid true vertical to molar reduced to 16mm, suggesting distal molar movement. ([Figure 9]).
Two year post-retention photographs ([Figure 10], [Figure 11]) and Lateral cephalogram ([Figure 12]) shows well settled balanced occlusion without any relapse, occlusion is better than post-treatment records which imply the success of our treatment.
Conclusion
It was discovered that the modified M Pendulum appliance was a very effective, non-invasive diatlization technique that didn't require patient compliance. In just 4 months, molar distalization of 3.5 mm and 4 mm on the left and right sides, respectively, was accomplished, as well as Class I molar and canine connection. In this instance, we were successful in achieving competent lips and attractive soft tissue harmony and balance.
Source of Funding
None.
Conflict of Interest
None.
References
- M F Sfondrini, V Cacciafesta, G Sfondrini. Upper molar distalization: a critical analysis. Orthod Craniofac Res 2002. [Google Scholar]
- B Melsen. Effects of cervical anchorage during and after treatment: an implant study. Am J Orthod 1978. [Google Scholar]
- A A Gianelly, A S Vaitas, W M Thomas. The use of magnets to move molars distally. Am J Orthod . [Google Scholar]
- WL Wilson. Modular orthodontic systems.. J Clin Orthod 1978. [Google Scholar]
- WL Wilson. Modular orthodontic systems. Part 2. J Clin Orthod 1978. [Google Scholar]
- A Carano, M Testa. The distal jet for upper molar distalization. J Clin Orthod 1996. [Google Scholar]
- G Scuzzo, F Pisani, K Takemoto. Maxillary molar distalization with a modified pendulum appliance. J Clin Orthod 1999. [Google Scholar]
- DA Covell, DW Trammell, RP Boero, R West. A cephalometric study of Class II division 1 malocclusions treated with the Jasper Jumper appliance. Angle Orthod 1999. [Google Scholar]
- JJ Hilgers. The pendulum appliance for Class II non-compliance therapy. J Clin Orthod 1992. [Google Scholar]
- N Cetlin. Ten Hoeve A. Nonextraction treatment. J Clin Orthod 1983. [Google Scholar]
- F Angelieri, RR Almeida, MR Almeida. Dentoalveolar and skeletal changes associated with the pendulum appliance followed by fixed orthodontic treatment. Am J Orthod Dentofac Orthop 2006. [Google Scholar]
- A Caprioglio, M Cozzani, M Fontana. Comparative evaluation of molar distalization therapy with erupted second molar: segmented versus quad pendulum appliance. Prog Orthod 2014. [Google Scholar] [Crossref]
- TJ Bussick, JA Mcnamara. Dentoalveolar and skeletal changes associated with the pendulum appliance. Am J Orthod Dentofac Orthop 2000. [Google Scholar]
- FK Byloff, MA Darendeliler. Distal molar movement using the pendulum appliance. Part 1: clinical and radiological evaluation. Angle Orthod 1997. [Google Scholar]
- JC Asensi, V Kalra, M Fontana, M Cozzani, A Caprioglio. Non-compliance maxillary molar distalizing appliances: an overview of the last decade. J Clin Orthod 2001. [Google Scholar]