- Visibility 84 Views
- Downloads 12 Downloads
- DOI 10.18231/j.jco.2024.020
-
CrossMark

Advansync in management of class II malocclusion: A systematic review
- Author Details:
-
 Mansee Lodd *
Mansee Lodd *
-
Ravindranath V.K
-
Anjali Gheware
-
Amol Mhatre
-
Navin Wadhwani
-
Neeraj Kolge
Introduction
In the nineteenth century, malocclusion was thought to represent an abnormal state, but by the mid-twentieth century Orthodontists questioned whether malocclusion was a malady or a malformation. Over the next century Orthodontists recognised malocclusion to represent a malformation and more often an anatomical variation.[1]
Several methods to classify malocclusion were described but the one described by Dr. Edward Angle in 1898 is still widely used. Angle defined three classes of malocclusion based on the antero-posterior relationship of the upper and lower occlusal segments. They were as follows; Class I in which there is a normal antero-posterior relationship; Class II in which the mandibular buccal segments are distal to those of the maxilla and Class III in which they are mesial.
Class II malocclusions are further divided into two categories: division 1 in which there is an excessive overjet; and division 2 in which the upper central incisors are retroclined, the overbite is greater than normal and the overjet normal.[2]
Although the classification was established, the etiology was not fully understood. This lacuna was then filled by Mcnamara Jr. in 1981 as he diagnosed the Class II etiology in which the most prevalent component was the skeletal retrusion of the mandible.[3], [4]
It comes as no surprise that Class II malocclusions are of interest to the practising Orthodontists since they constitute a significant percentage of the cases they treat.
In individuals with normal occlusion and skeletal relationship, the amount of maxillary and mandibular growth is synchronized and the result is a well-balanced and esthetically pleasing profile. But with respect to individuals with Class II malocclusions, there is an anteroposterior discrepancy between the maxillary and mandibular dentitions, which may or may not be accompanied with a skeletal discrepancy. To better understand the success of the treatment of this malocclusion it is important to understand if the individual is in the stage of active growth or has completed growth. If the patient presents with the former then the clinician has the benefit of utilising the growth changes of the maxilla and mandible to a great extent. The most favourable treatment options for growing patients include using functional appliances which enhance mandibular growth (mandibular advancement) and headgears, that provide extra oral force to restrict further maxillary growth or combination of both.[5]
The correction of Class II malocclusion with removable appliances such as the twin block requires patient compliance. This dependency on patient compliance slowed down treatment progress in non-compliant patient thereby spawning the need for fixed functional appliances. The introduction of fixed functional appliance by Dr. Emil Herbst – the Herbst appliance led to the development of an array of fixed functional appliances. These appliances are used all day which causes a continuous incentive force for mandibular growth. The mechanism of mandibular adaptation is similar to that of removable appliances with the difference being that it is tooth borne and exerts its effects to the underlying bone via teeth by transmitting the forces developed as a result of the continuous forward posturing of the lower jaw.[6]
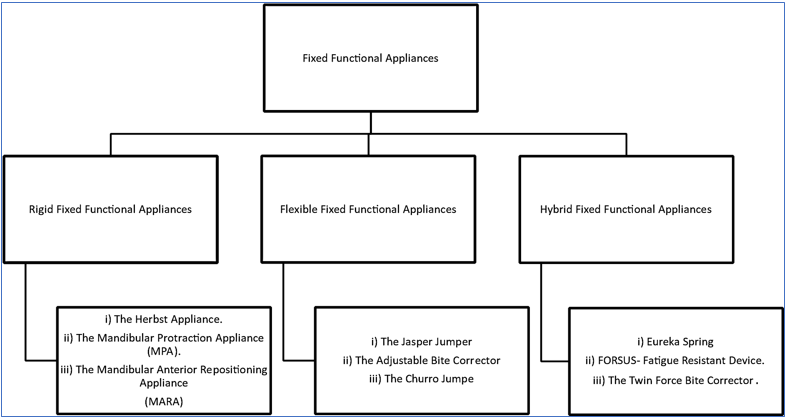
These appliances are classified into rigid, flexible, and hybrid fixed functional appliances. Rigid fixed functional appliances restrict mandibular movement and flexible fixed functional appliances have a frequency of breakage. These shortcomings led to the improvisation of “Hybrid fixed functional appliances”. Amidst the various appliances Forsus Fatigue Resistant Device™ (3M Oral Care, USA), Powerscope™ (American Orthodontics, USA) are widely used by clinicians.
The advent of Advansync™ (Ormco, USA) by Terry and Bill Dischinger in 2008 led to the introduction of a new fixed functional appliance with the ability to correct the class II malocclusion from the very first appointment. Modelled on the original Herbst appliance but smaller in size making it easier to place, activate and remove. This ability led to reduction in treatment time by almost six months.[7]
The development of another fixed functional appliance caused a shift in attention from the older appliances. This led to the question of whether Advansync™ is truly an exclusive appliance or another run of the mill appliance. This systematic review aims to understand that very question.
Objective
Does Advansync improve the dental, skeletal and soft tissue parameters in patients presenting with Class II malocclusion?
Materials and Methods
Protocol and registration
The systematic review protocol was registered at the international prospective register of systematic reviews (PROSPERO- CRD42022354682) and performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis – Diagnostic Test Accuracy (PRISMA- DTA) checklist (Salameh et al., 2020).
Also, it is available at the following link.
https://www.crd.york.ac.uk/prospero/
Inclusion and Exclusion Criteria
|
Criteria |
Description |
|
P: Population |
Patients with Class II malocclusion with retruded mandible in the age group of (10-16) years of age and with no medical history . |
|
I: Intervention |
Advansync, a class II corrector. |
|
C: Comparison |
Powerscope, Twin block, intermaxillary elastics, MARA, Forsus fatigue resistant device and also with cases with Orthodontic treatment without fixed functional appliance . |
|
O: Outcome |
Improvement in skeletal, dental and soft tissue parameters in patients undergoing Class II correction with Advansync. |
|
Criteria |
Description |
|
Study type |
In-vivo studies comparing the efficiency of Advansync with other fixed functional appliances. |
|
Publication type |
Randomized clinical trial, retrospective clinical trial and case reports |
|
Publication date |
Studies published from January 2001 to July 2022. |
|
Criteria |
Description |
|
Study type |
Animal studies, In-vitro studies, surveys and questionnaire based studies |
|
Publication date |
Studies published before January 2001 |
Data Sources and Searches
Electronic search of PubMed (including MEDLINE), EBSCO Host & Google Scholar search engine for articles published from 1st January 2000 to 31st July 2022 was conducted.
The terms mentioned in the concept table were used to formulate a search strategy. The terms were combined using suitable Boolean operators (AND, OR, NOT). A similar search strategy was applied in all the three electronic searches.
The search strategy for the PubMed, Ebsco Host and google scholar database has been mentioned in following tables and figures.
The English language and the time limit filters were used at the end as search limits.
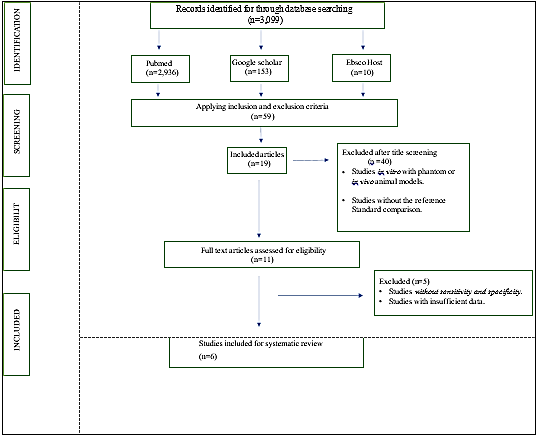
Out of the 3,099 articles obtained, 2,936 were obtained from Pubmed, 10 were obtained from Ebsco Host database and 153 articles from google scholar search engine respectively.
|
Population |
“Class II malocclusion *”[tiab]OR “Class II malocclusions” [tiab] OR “Angles Class II” [Mesh]OR “distocclusion” [Tiab]OR “Class II Skeletal malocclusions*”[tiab] OR “Class II Skeletal malocclusion”[tiab]OR “distocclusion”[tiab] |
|
Intervention |
“AdvanSync*” [tiab] OR “ Advansync 2” [tiab] |
|
Comparison |
Powerscope[tiab] OR Twin block [tiab] OR intermaxillary elastics [tiab] OR MARA[tiab] OR Forsus fatigue resistant device [tiab] OR EVAA appliance[tiab] OR Herbst appliance [tiab] OR Jasper Jumper [tiab] OR Vektor Pro [tiab] |
|
Outcome |
Comparative evaluation [tiab] |
|
Combined Search |
Class II malocclusion [tiab] OR Class II malocclusion [tiab] OR Angles Class II OR distocclusion [tiab] OR Class II Skeletal malocclusions [tiab] OR Class II Skeletal malocclusion [tiab] OR distocclusion [tiab] AND AdvanSync [tiab] OR Advansync 2 [tiab] Powerscope[tiab] OR Twin block [tiab] OR intermaxillary elastics [tiab] OR MARA[tiab] OR Forsus fatigue resistant device [tiab] OR EVAA appliance[tiab] OR Herbst appliance [tiab] OR Jasper Jumper [tiab] |
Data extraction
For all included studies, following descriptive study details were extracted by two independent reviewing authors (and ) using pilot-tested customized data extraction forms: Study ID, Author Year of publication, Study Design, sample characteristics (study population), intervention characteristics (type of class II corrector used) and main study results like changes in mandibular proclination, maxillary retroclination, increase in the incisal mandibular plane angle, change in molar relationship, and changes in facial profile was noted. The corresponding authors were contacted via email where further information was needed.
Study selection
A total of 59 articles that were obtained through electronic searches were exported into the Mendeley Desktop software.
The ‘check for duplicates’ feature of this software was then used to identify and eliminate duplicates. Each article that was detected as a duplicate by the Mendeley Desktop software was checked meticulously. The articles were thoroughly evaluated for their Title, Author Name, Publication Journal, Issue, and Year. After thorough checking, the ‘Merge duplicates’ feature was used to merge the duplicate articles. 19 articles were left after the elimination of duplicates and were subsequently taken into further consideration for the data selection process.
Steps of data selection as follows:
Two calibrated reviewers independently screened the relevant titles of the studies found through the electronic search. In case of any doubt, the study was included for further screening in the next stage. Out of 59 articles, 40 articles were excluded after screening of the title. The articles thus eliminated were either literature reviews, pilot study, case reports, case series. Both reviewers agreed on elimination of these articles since they contained data that was irrelevant to this systematic review. Thus, 19 articles were obtained after title screening.
Two calibrated reviewers now independently reviewed the full texts of the studies found relevant after the title and abstract screening. Out of the 19 articles, only 6 articles met the inclusion criteria and were thus included in this systematic review. Authors of the included studies were contacted in case of any missing data.
Discussion among reviewers was done if there were any disagreements. A third reviewer was called in for a final decision, if any disagreement over article selection persisted between the two calibrated reviewers.
A descriptive summary of data selection has been put forth in the PRISMA Flowchart i.e. PRISMA 2009 Flow Diagram.
Risk of Bias
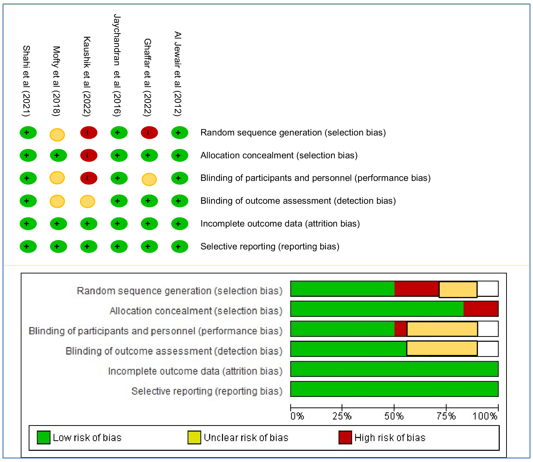
To assess the methodological quality and applicability of the included ROBINS-I (Risk of Bias in Non-Randomised studies of interventions) tool was applied.
Two authors independently evaluated the quality of each included study under two domains viz. patient selection, performance of device, ; and scored each signalling questions under the domains as “yes”, “no” and “unclear”.
Risk of bias summary and applicability concern was graphically plotted using Review Manager (RevMan) software version 5.3.
Discussion
The complexity and multifactorial etiology of Class II malocclusion cause the treatment of such malocclusions an enigma to Orthodontists. The malocclusion caused could be due to improper positioning of the maxilla or the mandible, the mandibular retrognathia being a more common finding. This shifted the focus of treatment to advancing the position of the mandible although restricting the maxillary growth also provides a positive effect in the treatment of Class II malocclusion.[8]
The etiology of Class II malocclusion is considered to be multifactorial wherein genetic factors and environmental factors play a major role. Lundström reported that in monozygotic twins there was a 68% concordance of having a Class II malocclusion; on the other hand, dizygotic twins had a 24% concordance.[9]
In terms of the environmental factors, the early loss of maxillary second deciduous molars in a patient with an otherwise Class I occlusion could result in the mesial migration, rotation and tipping of the maxillary first molars, and the creation of a Class II malocclusion. In patients with a persistent Finger sucking habit and excessive overjet, the lower lip may become trapped behind the maxillary incisors, causing abnormal contraction of the mentalis and other perioral muscles leading the maxillary incisors to further tip labially. Therefore, persistent finger, tongue, or lip habits can either result in a Class II malocclusion or accentuate an existing one.[10], [11]
The treatment of Class II malocclusions began in the 1800s when Norman William Kinglsey introduced his vulcanite plate and introduced the concept of “jumping the bite” for correction of mandibular position. This was followed by the work of Wilhelm Roux who studied the natural forces and functional simulation on form giving rise to the concept of Functional Jaw Orthopedics which is based on the enhancement of mandibular growth during peak growth. Thus began the development of numerous functional appliances but it was Viggo Andresens Activator that gained widespread clinical use.
Although the appliance provided a paramount difference in treatment it was highly patient compliant.
To overcome this drawback, Dr. Emil Herbst introduced his appliance at the 5th International Dental Congress in Berlin in 1909. This was a major development in the world of functional appliances but was overlooked till Panchers reintroduced it in 1970s. Thus began the era of fixed functional appliances in the world of orthodontics with over twenty fixed functional appliances available today.
Before we discuss the results of the systematic review it is important to understand the types of fixed functional appliances. A classification of these appliances was given by Ritto AK et al in 2000 and is the most commonly used classification for fixed functional appliances
In the current systematic review, a total of six articles were selected based on our inclusion and exclusion criteria. The articles were assessed for the risk of bias under different domains thereby allowing us to understand the validity of the study.
The MARA™ (Mandibular Anterior Repositioning Appliance) developed by Dr. D Toll and modified in 1994 by Dr. James E Eckhart functions as a fixed non-compliance appliance to correct Class II malocclusions. A study titled ‘A comparison of the MARA™ and the Advansync™ functional appliances in the treatment of Class II malocclusion’ carried out by Al-Jewair et al in 2012 discussed the effects of both the appliances on the mandible. The study concluded that MARA produced a significant elongation in the total length of the mandible whereas the AdvanSync™ caused a pronounced headgear effect with the net result that both appliances resulted in similar skeletal and dentoalveolar findings. Since there is a low risk of bias in the study, the results are considered to be accurate making it of high clinical relevance.[12]
Intermaxillary elastics have been used for correction of Class II and Class III malocclusions along with the correction of midline discrepancies as well. They are simple to use, economical and effective but are highly patient-compliant. Thus a study was carried out to understand the effectiveness of AdvanSync™ when compared with Intermaxillary elastics in the correction of Class II elastics by Jayachandran et al in 2016. The study results stated that while AdvanSync™ corrected the Class II malocclusion through maxillary skeletal growth restriction and mandibular dentoalveolar changes whereas with intermaxillary elastics changes were seen in both maxilla and mandible. The low risk of bias leads to acceptance of the results without questioning the validity of the study. [13]
Nickel Titanium (NiTi) coil springs maybe a better substitute to intermaxillary elastics as they generate lower and more continuous forces that are affected to a lesser degree with humidity and pH. This characteristic of better force maintenance may cause faster and more physiologic movement with minimal aggression to dental and periodontal tissues. A study comparing the dentoskeletal changes seen with AdvanSync™ and Intermaxillary coil springs was done by Mofty et al in 2018. The results spoke about the effects of both wherein both treatment modalities produced vertical changes by increasing the anterior facial height. They also produced retroclination of upper incisors, proclination of lower incisors thereby improving the overjet and molar relationship. The study concluded by stating that Intermaxillary coil springs produced more dentoalveolar improvements than Advansync™ although they suggested that Advansync™ was more suitable for non-compliant patients than intermaxillary coil springs as less patient co-operation was needed. An unclear selection and performance bias introduces the possibility of inaccurate results. Hence further studies need to be done to understand the effectiveness of both groups in a better manner.[14]
The most conventional removable appliance used in Class II correction is the Twin Block appliance introduced by William Clark. It acts by promoting mandibular growth, restricting further forward growth of the maxilla and improving skeletal relationships in individuals with mandibular retrusion. An observational retrospective study was carried out by Shahi et al in 2021 to understand the effectiveness of Advansync™ in comparison with the traditional twin block. The authors concluded that both the appliances resulted in similar skeletal, dentoalveolar, and soft tissue changes. In a similar study carried out by Ghaffar et al in 2022, it was found that the appliances produced similar effects in the sagittal plane but some maxillary restriction was observed for AdvanSync2™ appliance although there was a significant lower incisor proclination in the AdvanSync™ group along with a clockwise rotation of the mandible. The verticals were maintained in the twin block group by sequential trimming as and when required. Hence, twin block can be used to inhibit vertical development, while AdvanSync2™ can be used to produce significant mandibular changes in individuals with post pubertal growth past peak height velocity. The former study presents with a low risk of bias but the latter presents with a high risk of selection bias thereby more care should be taken to avoid this for future studies.[15], [16]
Lastly comparing the original Herbst appliance to its modification which is the Advansync™ appliance in a randomized control trial, Kaushik et al.[17] have reported that there was a significant increase in the mandibular length as well as a reduction of the total overjet. In both these parameters, the Herbst appliance produced better results as compared to the Advansync™ appliance although the latter produced significant lower incisor proclination. The above mentioned study presented with a high risk of selection bias in terms of random sequencing and allocation concealment as well as a high risk of performance bias in which blinding of participants and personnel were not carried out to the set standard. Thus this leads us to question the validity of the study and further research is required for the same.[17]
The clinical implications of Advansync™ include increased patient compliance along with reduced treatment time. Due to the reduced size, there is a significant reduction in breakage. It should be noted that according to majority of the studies, the use of Advansync™ causes maxillary restriction due to the headgear effect and thereby a pseudo mandibular advancement is claimed.[18]
Advansync™ showed a significant clockwise rotation of the functional occlusal plane resulting in mandibular incisor proclination of up to 5° which needs to be controlled. This negative effect can be controlled by torquing the mandibular incisors
Since Advansync™ causes increased proclination of mandibular incisors, the author suggests that Advansync™ be used early in treatment prior to the fixed appliance to prevent the deleterious effect of the fixed functional appliance on the functional occlusion plane and increased mandibular incisor proclination
Scope for Future Research
The scope for future research is as discussed below.
A controversy regarding the headgear effect of Advansync™ along with pseudo mandibular advancement persists. This calls for future studies to better investigate and give a conclusion on the same. The author recommends studies with a larger sample size of equal gender distribution along with homogenous growth stages of participants to ensure the study is more reliable as growth plays a very important role in the final results using functional appliances.
Follow-up of the cases till the end of fixed treatment and into the post-retention phase is of utmost importance to the practising orthodontist as it helps to understand the long-term stability of the results obtained from using Advansync ™. This lacunae in research should be addressed for a better understanding of the long-term stability of the correction obtained.
Ethical considerations prevent the utilization of a concurrent control group in the majority of studies of functional appliances. Consequently, a historical control sample is usually employed, which may not necessarily mirror the experimental group in terms of growth pattern. Thus studies are operated under the assumption that the growth trajectory of the controls followed a linear pattern and corresponds to that of the experimental groups. However, the clinical outcomes observed in cephalometric studies. Cannot be solely attributed to the effects of growth modification by the appliances under examination. Further exploration of other factors, employing alternative evaluation methods such as tomographic studies of the temporomandibular joints maybe warranted.
Conclusion
The advent of the fixed functional appliances has improved the effectiveness of treatment in Class II malocclusions, especially in non- compliant patients. The availability of various fixed functional appliances today allows the Orthodontists to choose from an array of appliances. This systematic review was done on Advansync (Ormco, USA). The appliance has the benefit of being introduced very early in the treatment, along with minimal size which reduces breakage of the fixed appliance as well as increases patient comfort. However, it is understood that there is a higher headgear effect on the maxilla than forward movement of the mandible with the use of this appliance thereby causing a pseudo-effect on mandibular advancement. The increase in the proclination of the lower incisors is an unavoidable side-effect seen with the use of Advansync. According to the results of this systematic review on comparison of AdvansyncTM to other functional correctors presented with comparable changes in the skeletal, dental and dentoaloveolar components.
To conclude, increased patient comfort along with reduced treatment time gives Advansync TM an edge over other fixed functional appliances.
Source of Funding
None.
Conflict of Interest
None.
References
- LW Graber, RL Vanarsdall, KWL Vig. . Orthodontics: Current Principles and Techniques 2012. [Google Scholar]
- J. F. Gravely M.Ch.D., D.Orth. R.C.S., L.D.S. D. B. Johnson B.D.S., F.D.S., D.Orth. . . [Google Scholar]
- J A Mcnamara. Components of Class II malocclusion in children 8-10 years of age. Angle Orthod 1981. [Google Scholar]
- Cozzap, Baccettit, Detoffoll Franchil. McNamaraJA Mandibular changes produced by functional appliances in Class II malocclusion: a systematic review. Am J Orthod Dentofacial Orthop 2006. [Google Scholar]
- T Bajaj, N Potode, A Verulkar. . Int J Orthod Rehabil 2019. [Google Scholar]
- M Graber T, T Rakosi, Petrovic Alexandre G. . Dentofacial orthopedics with functional appliance.2thEdn. Mosby Ltd 2009. [Google Scholar]
- P Cozza, T Baccetti, L Franchi, De Toffol, J Mcnamara. Mandibular changes produced by functional appliances in Class II malocclusion: a systematic review. Am J Orthod Dentofac Orthop 2006. [Google Scholar]
- AK Chauhan, F Alam, S Verma, S Shafaq. Fixed functional appliances for correction of Class II malocclusion: A review. Int J Orthod Rehabil 2021. [Google Scholar]
- A Lundström. . Tooth Size and Occlusion in Twins 1948. [Google Scholar] [Crossref]
- SE Bishara. Class II malocclusions: diagnostic and clinical considerations with and without treatment. In Semi Orthod 2006. [Google Scholar]
- TM Graber. The three M’s: muscles, malformation and malocclusion. Am J Orthod 1963. [Google Scholar]
- Al Jewair Ts Preston, CB Moll, EM Dischinger. A comparison of the MARA and the AdvanSync functional appliances in the treatment of Class II malocclusion. . The Angle Orthod 2012. [Google Scholar]
- S Jayachandran, WA Wiltshire, SM Hayasaki, FH Pinheiro. Comparison of AdvanSync and intermaxillary elastics in the correction of Class II malocclusions: A retrospective clinical study. Am J Orthod Dentofac Orthop 2016. [Google Scholar]
- MH El Mofty, SA Ibrahim, OS El-Shall, WA Tawfik. Evaluation of dentoskeletal changes accompanying the treatment of class II malocclusion by Advansync appliance versus intermaxillary coil spring mechanics.. Al-Azhar Dent J Girls 2018. [Google Scholar]
- AK Shahi, P Sharma, A Juneja, D Shetty, R Bhardwaj, S Jain. Comparison of Advansync2® and twin block appliances in treatment of class II malocclusion with retrognathic mandible-an observational retrospective study. J Indian Orthod Soc 2022. [Google Scholar]
- F Ghaffar, JA Akhtar, O Mughal, AT Shahid, R Shafique, HZ Bibi. Comparative Analysis of Dentoskeletal Changes of the Twin Block Appliance and the AdvanSync2 Appliance in Treatment of Skeletal Class-II Malocclusion in Pakistani Population: A Randomized Clinical Trial.. Angle Orthod 2012. [Google Scholar]
- K Kaushik, MS Sidhu, S Grover, A Dabas, N Dogra, J Nindra. Comparative Three Dimensional Evaluation of Dentoskeletal Parameters using AdvanSync & Herbst Appliance in Class II Malocclusion: “A Randomized Controlled Trial”. World J Dent 2022. [Google Scholar]
- P Raghav, S Mathur, K Amit, S Mohan. Therapeutic effectiveness of AdvanSync2 at different stages of skeletal maturity in skeletal class II malocclusion: a single-blind clinical trial.. APOS Trends Orthod 2020. [Google Scholar]