- Visibility 37 Views
- Downloads 11 Downloads
- DOI 10.18231/j.jco.2025.006
-
CrossMark

Radiographic assessment of apical root resorption in the mandibular molars following the usage of resin bite turbos in orthodontic patients– A retrospective study
- Author Details:
-
Rebekah Raju
-
 Ramasamy Navaneethan
Ramasamy Navaneethan
-
Aravind Kumar Subramanian
-
Karthikeyan Ramalingam
-
Hande Uzunçıbuk *
-
Maria Maddalena Marrapodi
-
Diana Russo
-
Marco Cicciù
-
Giuseppe Minervini
Introduction
Orthodontic therapy involves the use of bite turbos, bite planes, or bite blocks in the treatment of malocclusions such as deep bite, scissor bite, crossbite, and other centric relation discrepancies.[1] Depending on the kind of correction needed, these bite blocks can be utilized in the anterior or posterior regions. Anterior bite turbos are used in situations involving deep bite and anterior crossbite, whereas posterior bite turbos are used in situations involving open bite and posterior crossbite. They can be composed of composite restorations, metal, glass ionomer cement, or acrylic. Resin turbos were more widely used due to the shortcomings of the metal and other materials [2]
Bite turbos are frequently utilized in orthodontic therapy to disocclude the lower and upper teeth to achieve adequate alignment and leveling. Still, there may be several negative effects associated with long-term use of the same. Tooth mobility, decline in vitality, intrusion and orthodontically induced root resorption are among the several drawbacks. [3], [4]
One major iatrogenic side effect of orthodontic treatment using resin bite turbos is reported to be root resorption (Han et al., 2005)[4] More recently, research endeavors have sought to understand better the causal connection among root resorption, tooth movement, and force application. [5], [6] Scanning electron microscopic tests revealed that the movement of the tooth was crucial for root resorption, which was force- and time-dependent. Intrusive movement proved to be the most predictive type of tooth movement for occurrence of apical root resorption. [7], [8], [9] Root resorption due to excessive intrusive forces was the main focus of earlier studies. [10], [11], [12], [13], [14] The degree of this pathology was based on the amount of force used for intrusion, according to several individual research. Therefore, biting turbos' prolonged application of force may be the source of these symptoms.
Typically, orthodontically caused root resorption exhibits no symptoms. Hence, routine radiographs are crucial for an early diagnosis. Historically, it has been measured linearly on bidimensional radiographs, or with three dimensional CBCT measurements. [15] However, the assessment of root resorption brought on by the temporary placement of bite turbos hasn't been studied before. The goal of the current study was to determine how much apical root resorption in the molar region was brought on by the placement of bite turbos using OPGs.
Materials and Methods
Study population
The current investigation utilised retrospective analysis of the records of patients who had previously visited the dental institution's orthodontic department. The patients included were between the ages of 18 and 45. A study conducted by Gay et al. was used to determine the sample size calculation utilising the G*power analysis (version 3.1) (Gay et al., 2017).[16] The estimated sample size was 27, but the total sample was taken as 30. The power and alpha threshold were adjusted to 80% and 0.05, respectively.
Selection criteria
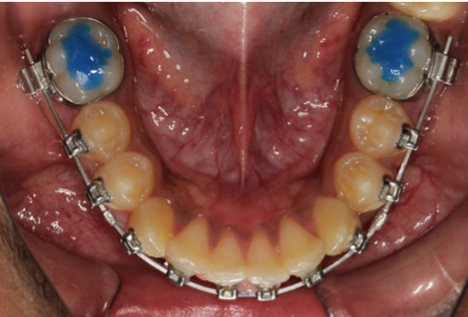
The selected sample consisted of a total of 30 OPGs of orthodontic patients, each before and after orthodontic therapy, for whom bite turbos were placed in the mandibular molar region for a minimum of 4 months during treatment ([Figure 1]). Patients whose orthodontic records were missing or who had endodontic therapy or apical root resorption at the pre-treatment stage were not included. Additionally, radiographs of poor quality were removed. Control groups were taken as the before and after OPGs of the patients without any placement of bite turbos during orthodontic treatment. Panoramic radiographs at both stages of orthodontic treatment (T0 and T1) were taken with the same setup.
Digital measurement
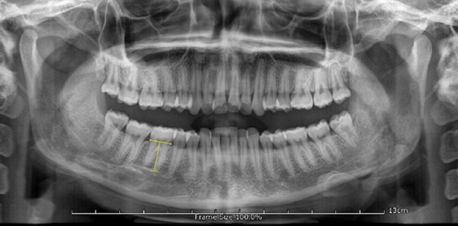
The FACAD digital software (ILEXIS, Sweden, version 3.12) was used to digitally measure the crown and root lengths ([Figure 2]). The root crown ratio (R/C) of the tooth was measured using the patients' digital OPG radiographs. The molar roots and crown lengths were measured using modified Lind approach (Lind, 1972).[17] As the measurements relied on relative ratios, there was no need to calibrate the images. The R/C ratio was calculated by dividing the length of the root by the crown length, as determined radiographically.
|
Groups |
Number of samples |
Relative crown ratio (%) |
Relative root ratio (%) |
rRCR ( Mean +/- SD ) |
|
Control group |
15 |
100.17 |
99.67 |
99.52+/-0.63 |
|
Study group |
15 |
100.11 |
96.69 |
96.58+/-1.79 |
|
Independent t-test |
F |
t |
Sig. (2-tailed) |
|
Between study and control groups |
6.875 |
5.963 |
0.014* |
|
Paired t-test |
Paired differences |
t |
Sig. (2-tailed) |
|
Before and after bite turbos |
0.268 |
5.238 |
0.001 * |
R/C ratio method
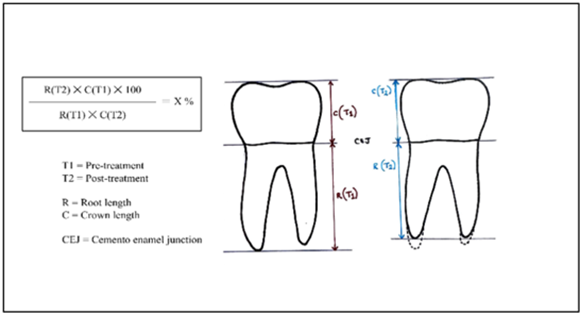
With the help of the modified Lind approach, a midpoint known as point M was drawn indicating the demarcation between the crown and root. An occlusal line was created in order to measure the molars, perpendicular to the tooth's long axis, connecting the molar cusps. The measurement of the crown was considered as the distance between the M point and the occlusal surface. The distance between the root apex and CEJ was used to calculate the root measurement. To draw the apical reference line, the apex of the longest buccal root was used. The relative changes in the crown root ratio (rRCR) were used for the calculation of root length. For every mandibular molar, corresponding ratio was determined for both pre-treatment and post-placement of blue bite for a minimum period of 4 months. Each of the mandibular molars was measured, and an average of the two was calculated before and after treatment. The rRCR was then calculated, as mentioned previously by Krieger et. al, by the formula shown in [Figure 3]. The rRCR of each tooth was measured for both groups and the mean was tabulated ([Table 1]). The rRCR was decreased when the root length was shortened during the treatment (Krieger et al., 2013).[18]
Statistical analysis
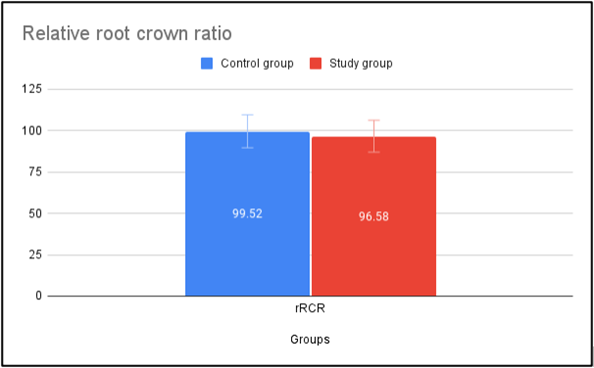
Data collection and analysis were conducted using SPSS® analysis software (Version 22). RCR and its fluctuations were calculated using the averages of the two measurements (Figure 4). The mean and standard deviation of quantitative measurements have been described in Table 1. The statistical significance between the study and control groups was determined by applying a t-test for independent samples, as specified in [Table 2].
Results
The statistical analysis of the rRCR before and after therapy revealed a decrease in rRCR, indicating a reduced length of the tooth roots. [Table 2] indicated that there was a significant difference (p=0.014) determined statistically between the study and control group ratios. The pre and post-ratio differences within the study groups were also significant (p=0.001) as mentioned in [Table 3].
Discussion
The current investigation examined bite turbos' effects on the mandibular molars and their impact on root resorption. The change in root length following the placement of the blue bite was measured using the relative crown root ratio, which was a method used to quantify resorption in orthodontic patients. A significant decrease was found in the root length of the mandibular molars due to the occlusal placement of bite turbos (p=0.001). This caused an excessive intrusive force over a while on the corresponding molars, leading to orthodontically induced root resorption.
Bite turbos have been used for various orthodontic purposes. They have been mainly used for the disocclusion of maxillary and mandibular teeth for proper placement of brackets and leveling and aligning of the malaligned teeth. Posterior bite turbos have often been used in cases when bracket positioning becomes difficult due to inadequate space between the teeth.[17] In certain open bite cases, these posterior build-ups are used to bring about bite closure by posterior intrusion and anterior extrusion. On the contrary, deep bite cases could be corrected by the placement of anterior bite turbos which led to extrusion of the posteriors by bite opening.[18]
Previous studies have assessed various skeletal and dentoalveolar changes caused by the placement of bite turbos. Arturo et al. noticed notable improvements in the skeletal and dental structures after using posterior build-ups as a non-surgical treatment for the open bite. 1mm of molars were intruded and a 3.98 mm rise in overbite were noted [19] Al Zoubi et al found increased extrusion of posterior teeth and increased lower facial height in patients with anterior bite turbos (p<0.05).[18] The impact of a temporary bite turbo on the periodontium was studied by Arya et al. The mean probing depth of the mandibular first molar along with periodontal alterations increased significantly following the installation of bite turbos.[20], [21], [22], [23], [24], [25], [26], [27] Additionally, prior research has demonstrated that high points due to improper restorations could lead to modifications in the periodontium, such as increased periodontal pocket depths, bone loss, and an increase in tooth mobility, which may have a comparable effect as a result of the placement of biting turbos.[28], [29] On the other hand, there was no statistically significant difference in the vertical displacements of the first molars between the two groups, according to Aliaga et al.[30], [31]
Root resorption was found to be the most significant parameter in this current research. The change in the root length was evaluated by determining the relative crown-root ratio. There was a significant change between mandibular molar root length before and after the placement of bite turbos. Previous studies have investigated the effects of intrusion leading to root resorption. Increased apical mobility has been linked to increased resorption, according to Sehgal et al (Segal et al., 2004).[32], [33] Paetyangkul et al also concluded that root resorption rises with an increase in application time, regardless of the force used.[34] According to Heba E. Akla et al., the orthodontic intrusion was invariably accompanied by root resorption. Yet neither statistically nor clinically did increase the intrusive force's magnitude result in a greater quantity of root resorption.[33] Harris et al. also discovered a substantial rise when comparing the root resorption rates to the controls.[32]
Therefore, the incidence of root resorption has been proven to be linked with excessive tooth movements such as intrusion. On the other hand, no prior studies had examined the resorption of the roots caused by the intrusive effects of the biting turbos. Hence, the present study was executed to assess the radiographic alteration in the mandibular molar root lengths when subjected to intrusive forces due to the placement of bite turbos. It has been proven that usage of Bite turbos for a prolonged period can cause intrusion of posterior teeth and lead to root resorption. Therefore, early evaluation is necessary to determine the degree of resorption in orthodontic subjects.
Limitations
The main drawback in the present investigation was the time taken for consideration of the study. The timing for the placement of bite turbos was not standardized in the study. Hence further studies with standardised protocols with longer time durations are needed to confirm the present findings.
Conclusion
It can be concluded that the R/C ratio is significantly altered before and after the usage of bite turbos during orthodontic therapy. Hence, bite turbos can be considered as a factor that could cause root resorption if used for a prolonged period during orthodontic therapy.
Author Contributions
It has been presented as follows: R.R. and K.R. designed the research study. R.R., N.R., and A.K.S. performed the research. K.R., D.R. and M.C. analyzed the data. H.U., G.M. and MMM. wrote the manuscript. Editorial modifications were made to the manuscript with input from all authors. The final manuscript was read and approved by all writers.
Source of Funding
This study was not supported by external funds.
Conflict of Interest
The authors declare no conflict of interest.
Acknowledgement
Not applicable.
References
- ND Kravitz, G Jorgensen, S Frey, J Cope. Resin bite turbos. J Clin Orthod 2018. [Google Scholar]
- G Singh, H Gupta, A Rathi, D Bisht, V Goyal, K Singh. The Use of Bite Raisers in Orthodontic Treatment - A Review of Literature. . Acta Sci Dent Sci 2021. [Google Scholar]
- E Güray. Temporary bite raiser. J Clin Orthod 1999. [Google Scholar]
- G Han, S Huang, JW Von Den Hoff, X Zeng, AM Kuijpers-Jagtman. Root resorption after orthodontic intrusion and extrusion: an intraindividual study. Angle Orthod 2005. [Google Scholar]
- MA Casa, RM Faltin, K Faltin, FG Sander, A Chavez Ve. Root Resorptions in Upper First Premolars after Application of Continuous Torque Moment Intra-Individual Study. J Orofac Orthop Fortschritte der Kieferorthopädie 2001. [Google Scholar]
- RM Faltin, VE Arana-Chavez, K Faltin, FG Sander, A Wichelhaus. Root resorptions in upper first premolars after application of continuous intrusive forces. J Orofac Orthop Fortschritte Der Kieferorthopädie 1998. [Google Scholar]
- S Baumrind, EL Korn, RL Boyd. Apical root resorption in orthodontically treated adults. Am J Orthod Dentofac Orthop 1996. [Google Scholar]
- Di Stasio, D Romano, A Paparella, RS Gentile, C Serpico, R Minervini. How social media meet patients questions: YouTube review for mouth sores in children. J Biol Regul Homeost Agents 2018. [Google Scholar]
- G Minervini, R Franco, MM Marrapodi, LE Almeida, V Ronsivalle, M Cicciù. Prevalence of temporomandibular disorders (TMD) in obesity patients: A systematic review and meta-analysis. J Oral Rehabil 2023. [Google Scholar]
- T Xu, S Baumrind. The relationship between apical root resorption and orthodontic tooth movement in growing subjects. Zhonghua Kou Qiang Yi Xue Za Zhi 2002. [Google Scholar]
- K Ghadirinejad, CW Day, R Milimonfared, M Taylor, LB Solomon, R Hashemi. Fretting Wear and Corrosion-Related Risk Factors in Total Hip Replacement: A Literature Review on Implant Retrieval Studies and National Joint Replacement Registry Reports. Prosthesis 2023. [Google Scholar]
- I Pelivan, I Šeparović, M Vuletić, N Dulčić, D Gabrić. Radiological and Periodontal Evaluation of Stock and Custom CAD/CAM Implant Abutments-A One-Year Follow-Up Study. Prosthesis 2023. [Google Scholar]
- T Tanaka, S Hara, H Hendawy, HM El-Husseiny, R Tanaka, T Asakura. Development of Small-Diameter Artificial Vascular Grafts Using Transgenic Silk Fibroin. Prosthesis 2023. [Google Scholar]
- S Choi, YS Kang, Isl Yeo. Influence of Implant-Abutment Connection Biomechanics on Biological Response: A Literature Review on Interfaces between Implants and Abutments of Titanium and Zirconia. Prosthesis 2023. [Google Scholar]
- D Lunardi, T Bécavin, A Gambiez, É Deveaux. Orthodontically induced inflammatory root resorption: apical and cervical complications. J Dentof Anom Orthod 2013. [Google Scholar]
- G Gay, S Ravera, T Castroflorio, F Garino, G Rossini, S Parrini. Root resorption during orthodontic treatment with Invisalign®: a radiometric study. Prog Orthod 2017. [Google Scholar]
- HO Alsheikho, D Jomah. A Simple Technique to Fabricate Bite Turbos. J Indian Orthod Soc 2021. [Google Scholar]
- EM Al-Zoubi, KS Al-Nimri. A comparative study between the effect of reverse curve of Spee archwires and anterior bite turbos in the treatment of deep overbite cases: Angle Orthod. Angle Orthod 2022. [Google Scholar]
- A Vela-Hernández, R López-García, V García-Sanz, V Paredes-Gallardo, F Lasagabaster-Latorre. Nonsurgical treatment of skeletal anterior open bite in adult patients: Posterior build-ups. . Angle Orthod 2017. [Google Scholar]
- AS Prasad, A Sivakumar. Effect of Posterior Bite Raiser on Periodontium of Lower Molars in Orthodontic Patients. J Evol Med Dent Sci 2021. [Google Scholar]
- N Vaid, V Doshi, M Vandekar. What's “Trend”ing in Orthodontic literature?. Gale Acad Online 2016. [Google Scholar]
- ND Kravitz, B Dalloul, YA Zaid, C Shah, NR Vaid. What percentage of patients switch from Invisalign to braces? A retrospective study evaluating the conversion rate, number of refinement scans, and length of treatment. Am J Orthod Dentofac Orthop 2023. [Google Scholar]
- A Venugopal, N Vaid, SJ Bowman. Outstanding, yet redundant? After all, you may be another Choluteca Bridge!. Semin Orthod 2021. [Google Scholar]
- NR Vaid. Artificial Intelligence (AI) driven orthodontic care: A quest toward utopia? . Semin Orthod 2021. [Google Scholar]
- YJ Lee, YA Kook, JH Park, J Park, M Bayome, NR Vaid. Short-term cone-beam computed tomography evaluation of maxillary third molar changes after total arch distalization in adolescents. Am J Orthod Dentofac Orthop 2019. [Google Scholar]
- M Alseraidi, I Hansa, F Dhaval, DJ Ferguson, NR Vaid. The effect of vestibular, lingual, and aligner appliances on the quality of life of adult patients during the initial stages of orthodontic treatment. Prog Orthod 2021. [Google Scholar]
- Di Stasio, D Lauritano, D Gritti, P Migliozzi, R Maio, C Minervini, G. Psychiatric disorders in oral lichen planus: a preliminary case control study. J Biol Regul Homeost Agents 2018. [Google Scholar]
- ER Vickers, MJ Cousins, A Woodhouse. Pain description and severity of chronic orofacial pain conditions. Aust Dent J 1998. [Google Scholar]
- M Carossa, N Scotti, M Alovisi, S Catapano, F Grande, M Corsalini. Management of a Malpractice Dental Implant Case in a Patient with History of Oral Bisphosphonates Intake: A Case Report and Narrative Review of Recent Findings. Prosthesis 2023. [Google Scholar]
- A Del Castillo, A Janson, G Vilanova, L Cevidanes, L Yatabe, M Garib. hree-dimensional dentoalveolar changes in open bite treatment in mixed dentition, spurs/posterior build-ups versus spurs alone: 1-year follow-up randomized clinical trial. Sci Rep 2022. [Google Scholar]
- G Segal, P Schiffman, O Tuncay. Meta analysis of the treatment-related factors of external apical root resorption. Orthod Craniofac Res 2004. [Google Scholar]
- DA Harris, AS Jones, MA Darendeliler. Physical properties of root cementum: Part 8. Volumetric analysis of root resorption craters after application of controlled intrusive light and heavy orthodontic forces: A microcomputed tomography scan study. Am J Orthod Dentofac Orthop 2006. [Google Scholar]
- HE Akl, AR El-Beialy, MA El-Ghafour, AM Abouelezz, El Sharaby. Root resorption associated with maxillary buccal segment intrusion using variable force magnitudes. Angle Orthod 2021. [Google Scholar]
- A Paetyangkul, T Türk, S Elekdağ-Türk, AS Jones, P Petocz, MA Darendeliler. Physical properties of root cementum: Part 14. The amount of root resorption after force application for 12 weeks on maxillary and mandibular premolars: A microcomputed-tomography study. Am J Orthod Dentofac Orthop 2009. [Google Scholar]